Frantz Travis L, Everhart Joshua S, West Julie M, Ly Thuan V, Phieffer Laura S, Valerio Ian L
Departments of Orthopaedic Surgery (T.L.F., J.S.E., T.V.L., and L.S.P.) and Plastic Surgery (J.M.W.), The Ohio State University Wexner Medical Center, Columbus, Ohio.
Division of Plastic and Reconstructive Surgery, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts.
JB JS Open Access. 2020 May 6;5(2):e0067. doi: 10.2106/JBJS.OA.19.00067. eCollection 2020 Apr-Jun.
Orthopaedic trauma etiologies are a common cause for amputation. Targeted muscle reinnervation (TMR) is a technique aimed at reducing or preventing pain and improving function. The purpose of this study was to examine postoperative phantom limb pain and residual limb pain following TMR in orthopaedic trauma amputees. In addition, postoperative rates of opioid and neuromodulator medication use were evaluated.
Twenty-five patients (60% male) prospectively enrolled in a single-institution study and underwent TMR at the time of major limb amputation (48% nonmilitary trauma, 32% infection secondary to previous nonmilitary trauma, and 20% other, also secondary to trauma). Phantom limb pain and residual limb pain scores, pain temporality, prosthetic use, and unemployment status were assessed at the time of follow-up. The use of opioid and neuromodulator medications both preoperatively and postoperatively was also examined.
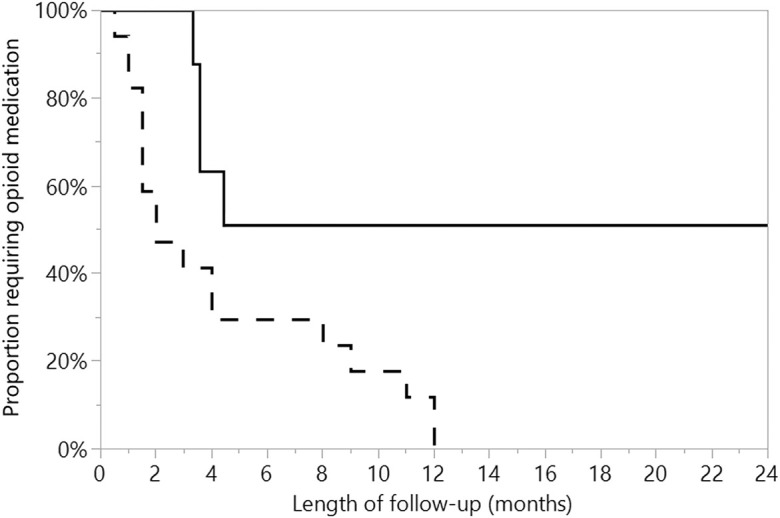
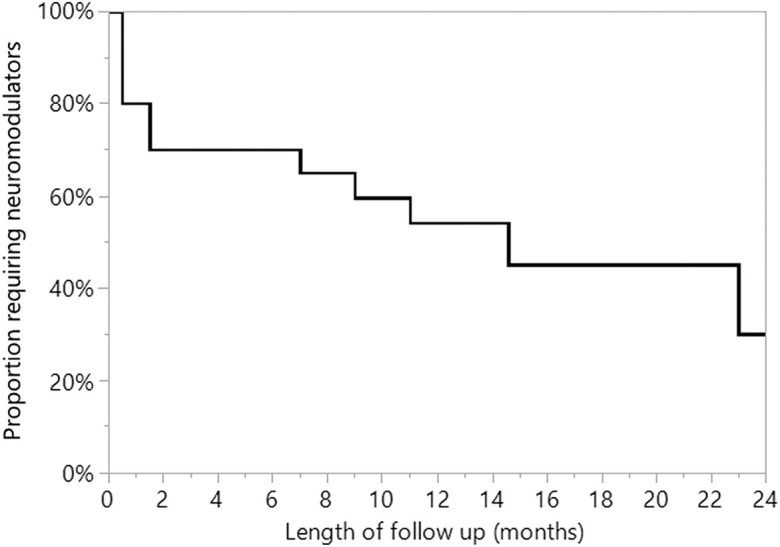
At a mean follow-up of 14.1 months, phantom limb pain and residual limb pain scores were low, with 92% of the patients reporting no pain or brief intermittent pain only. Pain scores were higher overall for male patients compared with female patients (p < 0.05) except for 1 subscore, and higher in patients who underwent amputation for infection (odds ratio, 9.75; p = 0.01). Sixteen percent of the patients reported opioid medication use at the time of the latest documented follow-up. Fifty percent of the patients who were taking opioids preoperatively discontinued use postoperatively, while 100% of the patients who were not taking opioids preoperatively discontinued postoperative use. None of the patients who were taking neuromodulator medication preoperatively discontinued use postoperatively (0 of 5). The median time to neuromodulator medication discontinuation was 14.6 months, with female patients taking longer than male patients (23 compared with 7 months; p = 0.02). At the time of the latest follow-up, the rate of reported prosthetic use was 85% for lower-extremity and 40% for upper-extremity amputees, with a rate of unemployment due to disability of 36%.
The use of TMR in orthopaedic trauma amputees was associated with low overall pain scores at 2-year follow-up, decreased overall opioid and neuromodulator medication use, and an overall high rate of daily prosthetic use.
Therapeutic Level IV. See Instructions for Authors for a complete description of levels of evidence.
骨科创伤病因是截肢的常见原因。靶向肌肉再支配(TMR)是一种旨在减轻或预防疼痛并改善功能的技术。本研究的目的是检查骨科创伤截肢患者接受TMR术后的幻肢痛和残肢痛。此外,还评估了术后阿片类药物和神经调节剂的用药率。
25例患者(60%为男性)前瞻性纳入一项单机构研究,并在大肢体截肢时接受TMR(48%为非军事创伤,32%为既往非军事创伤继发感染,20%为其他原因,也继发于创伤)。随访时评估幻肢痛和残肢痛评分、疼痛时间、假肢使用情况和失业状况。还检查了术前和术后阿片类药物和神经调节剂的使用情况。
平均随访14.1个月时,幻肢痛和残肢痛评分较低,92%的患者报告无疼痛或仅为短暂间歇性疼痛。除一个子评分外,男性患者的疼痛评分总体高于女性患者(p<0.05),因感染接受截肢的患者疼痛评分更高(优势比,9.75;p=0.01)。16%的患者在最新一次记录的随访时报告使用阿片类药物。术前服用阿片类药物的患者中有50%术后停药,而术前未服用阿片类药物的患者术后停药率为100%。术前服用神经调节剂的患者术后均未停药(5例中的0例)。停用神经调节剂的中位时间为14.6个月,女性患者停药时间长于男性患者(分别为23个月和7个月;p=0.02)。在最新一次随访时,下肢截肢患者的假肢使用率为85%,上肢截肢患者为40%,因残疾导致的失业率为36%。
骨科创伤截肢患者使用TMR与2年随访时总体疼痛评分较低、阿片类药物和神经调节剂总体用药减少以及日常假肢使用率总体较高相关。
治疗水平IV。有关证据水平的完整描述,请参阅作者指南。