Kim Sung Hwan, Oh Yong Seog, Choi Young, Hwang Youmi, Kim Ju Youn, Kim Tae Seok, Kim Ji Hoon, Jang Sung Won, Lee Man Young, Joung Boyoung, Choi Kee Joon
Division of Cardiology, Department of Internal Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
Division of Cardiology, Department of Internal Medicine, College of Medicine, St. Vincent's Hospital, The Catholic University of Korea, Seoul, Korea.
Korean Circ J. 2021 Jan;51(1):58-64. doi: 10.4070/kcj.2020.0174. Epub 2020 Sep 14.
Cavotricuspid isthmus (CTI) block is easily achieved, and prophylactic ablation can be performed during atrial fibrillation (AF) ablation. However, the previous study was too small and short-term to clarify the efficacy of this block.
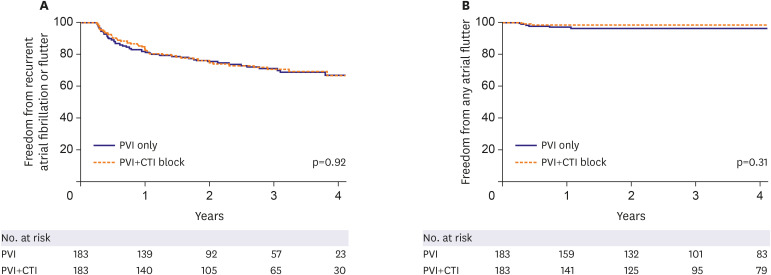
Patients who underwent catheter ablation for paroxysmal AF were enrolled, and patients who had previous or induced atrial flutter (AFL) were excluded. We randomly assigned 366 patients to pulmonary vein isolation (PVI) only and prophylactic CTI ablation (PVI vs. PVI+CTI).
There was no significant difference in procedure time between the two groups because most CTI blocks were performed during the waiting time after the PVI (176.8±72.6 minutes in PVI vs. 174.2±76.5 minutes in PVI+CTI, p=0.75). All patients were followed up for at least 18 months, and the median follow-up was 3.4 years. The recurrence rate of AF or AFL was not different in the 2 groups (25.7% in PVI vs. 25.7% in PVI+CTI, p=0.92). The recurrence rate of any AFL was not significantly different in the 2 groups (3.3% in PVI vs. 1.6% in PVI+CTI, p=0.31). The recurrence rate of typical AFL also was not different (0.5% in PVI vs. 0.5% in PVI+CTI, p=0.99).
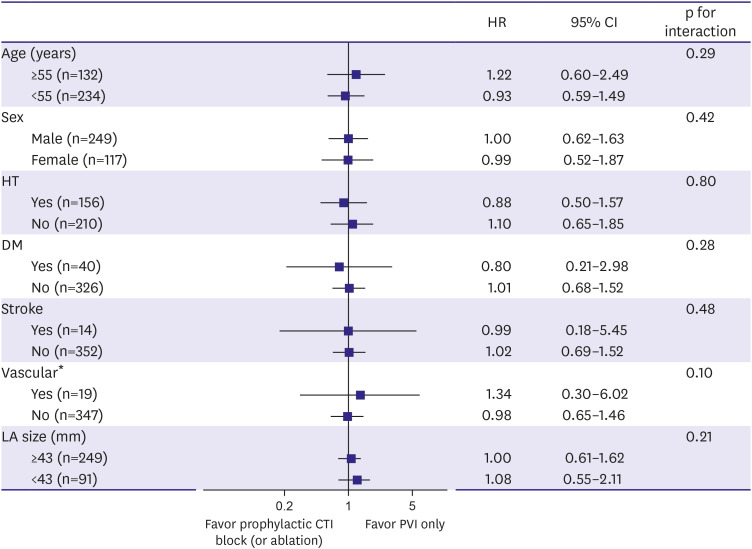
In this large and long-term follow-up study, prophylactic CTI ablation had no benefit in patients with paroxysmal AF without typical AFL.
ClinicalTrials.gov Identifier: NCT02031705.
三尖瓣峡部(CTI)阻滞易于实现,且可在心房颤动(AF)消融期间进行预防性消融。然而,既往研究规模过小且随访时间过短,无法阐明这种阻滞的疗效。
纳入接受阵发性AF导管消融的患者,排除既往有或诱发出心房扑动(AFL)的患者。我们将366例患者随机分为仅行肺静脉隔离(PVI)组和预防性CTI消融组(PVI对比PVI+CTI)。
两组手术时间无显著差异,因为大多数CTI阻滞是在PVI后的等待时间内进行的(PVI组为176.8±72.6分钟,PVI+CTI组为174.2±76.5分钟,p=0.75)。所有患者均随访至少18个月,中位随访时间为3.4年。两组AF或AFL的复发率无差异(PVI组为25.7%,PVI+CTI组为25.7%,p=0.92)。两组任何AFL的复发率无显著差异(PVI组为3.3%,PVI+CTI组为1.6%,p=0.31)。典型AFL的复发率也无差异(PVI组为0.5%,PVI+CTI组为0.5%,p=0.99)。
在这项大规模长期随访研究中,对于无典型AFL的阵发性AF患者,预防性CTI消融无益处。
ClinicalTrials.gov标识符:NCT02031705。