Wang Tao, Zhang Jinfu, Wang Wanxiang, Yang Xianwei, Kong Junjie, Shen Shu, Wang Wentao
Department of Liver Surgery and Liver Transplantation Center, West China Hospital of Sichuan University, Chengdu, People's Republic of China.
Department of Hepatobiliary, Pancreatic, and Splenic Surgery, The Affiliated Hospital of Inner Mongolia Medical University, Hohhot, People's Republic of China.
Cancer Manag Res. 2020 Nov 2;12:11015-11029. doi: 10.2147/CMAR.S272797. eCollection 2020.
There are few studies on the prognosis of elderly intrahepatic cholangiocarcinoma (iCCA) patients after liver resection. The aims of this study were to assess the cumulative incidences of cancer-specific mortality in elderly iCCA patients and to construct a corresponding competing risk nomogram for elderly iCCA patients.
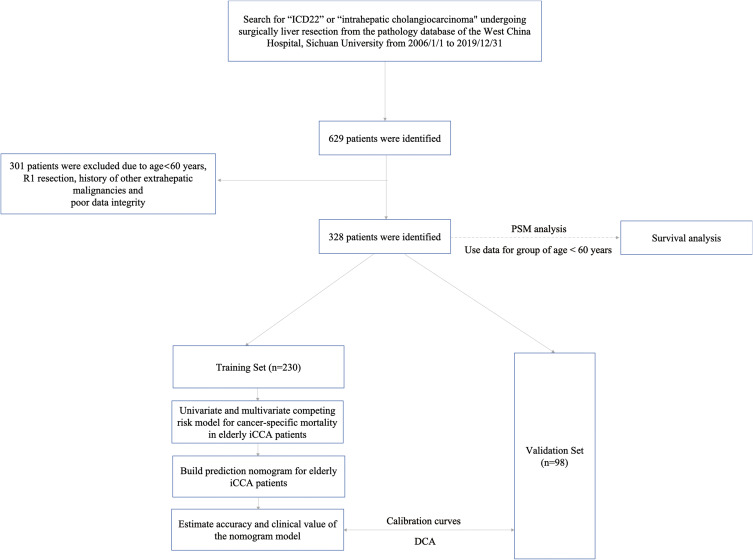
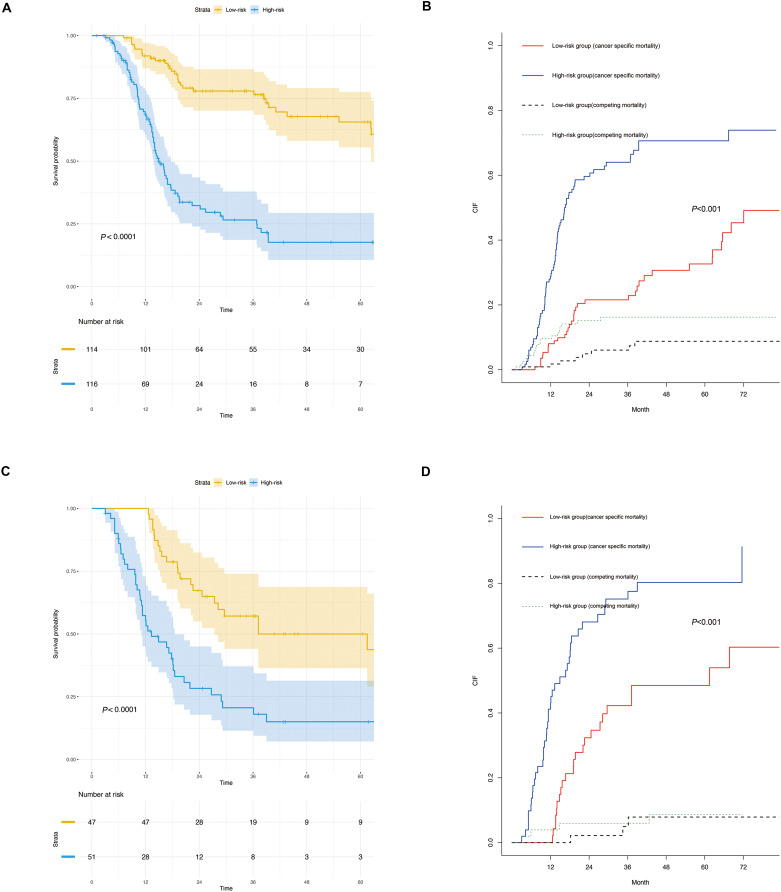
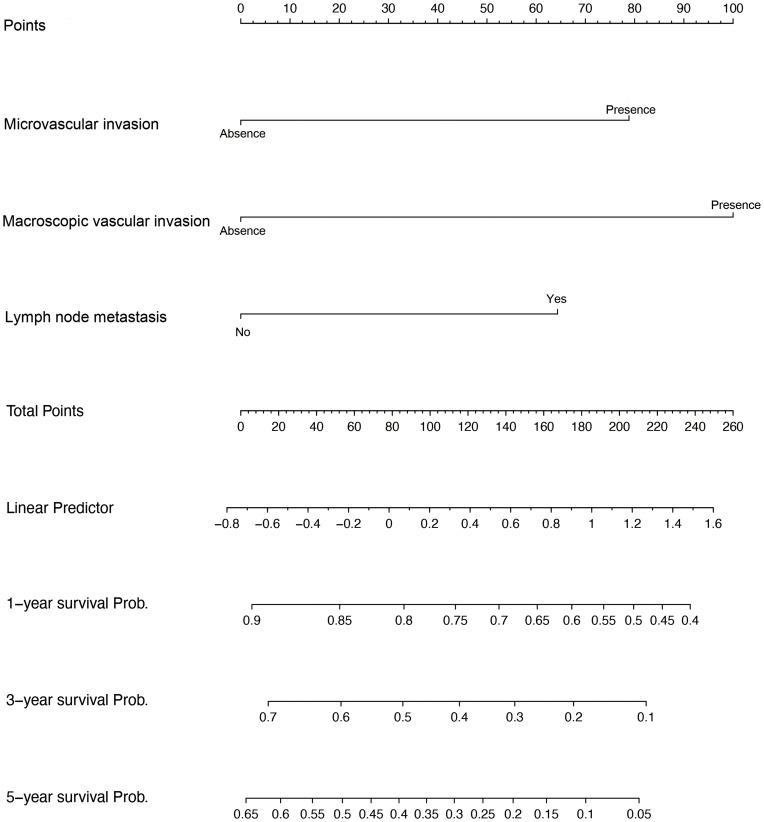
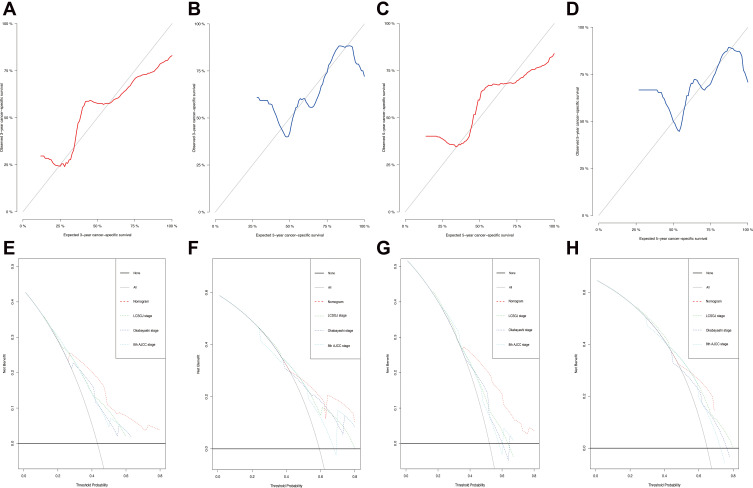
We performed a retrospective analysis of elderly patients with iCCA who underwent liver resection between January 2006 and December 2019. Eligible elderly iCCA patients were randomly divided into training and validation sets at a ratio of 7:3. Based on the results of multivariate analysis using the Fine-Gray competing risk model, we developed a competing risk nomogram using data from the training set to predict the cumulative probabilities of iCCA-specific mortality. The performance of the nomogram was measured by the concordance index (C-index) and calibration curves. To evaluate the clinical usefulness of the nomogram, the clinical benefit was measured by using decision curve analysis (DCA). Furthermore, the patients were categorized into two groups according to the dichotomy values of the nomogram-based scores, and their survival differences were assessed using Kaplan-Meier and cumulative incidence function (CIF) curves.
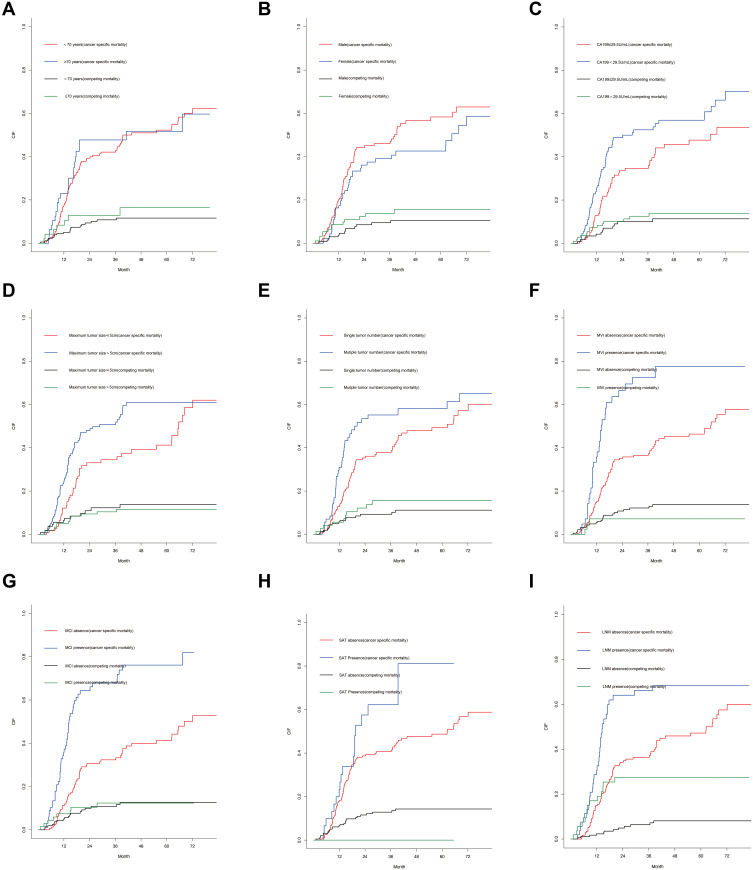
The 1-year, 3-year and 5-year cumulative iCCA-specific mortalities were 19.7%, 48.3% and 56.1%, respectively, for elderly iCCA patients. The multivariate Fine-Gray analysis indicated that microvascular invasion, macroscopic vascular invasion and lymph node metastasis were related to a significantly higher likelihood of iCCA specific mortality. The established nomogram was well calibrated and had a good discriminative ability, with a concordance index (C-index) of 0.742 (95% CI, 0.708-0.748). Furthermore, the DCA indicated that the nomogram had positive net benefits compared with the conventional staging systems. In the training set and validation sets, the high-risk group had the higher probabilities of iCCA cancer-specific mortality than the low-risk group; meanwhile, the patients in the high-risk the group had significantly poorer overall survival (OS) than those in the low-risk group.
Elderly iCCA patients had comparable long-term outcomes with non-elderly iCCA patients. In addition, we constructed a prognostic nomogram for predicting survival in elderly iCCA patients based on the competing risk analysis. The competing risk nomogram displayed excellent discrimination and calibration.
关于老年肝内胆管癌(iCCA)患者肝切除术后预后的研究较少。本研究的目的是评估老年iCCA患者癌症特异性死亡的累积发生率,并为老年iCCA患者构建相应的竞争风险列线图。
我们对2006年1月至2019年12月期间接受肝切除的老年iCCA患者进行了回顾性分析。符合条件的老年iCCA患者按7:3的比例随机分为训练集和验证集。基于使用Fine-Gray竞争风险模型的多变量分析结果,我们利用训练集的数据开发了一个竞争风险列线图,以预测iCCA特异性死亡的累积概率。列线图的性能通过一致性指数(C指数)和校准曲线来衡量。为了评估列线图的临床实用性,通过决策曲线分析(DCA)来衡量临床获益。此外,根据基于列线图评分的二分法值将患者分为两组,并使用Kaplan-Meier和累积发病率函数(CIF)曲线评估他们的生存差异。
老年iCCA患者1年、3年和5年的iCCA特异性累积死亡率分别为19.7%、48.3%和56.1%。多变量Fine-Gray分析表明,微血管侵犯、宏观血管侵犯和淋巴结转移与iCCA特异性死亡的可能性显著更高有关。建立的列线图校准良好,具有良好的鉴别能力,一致性指数(C指数)为0.742(95%CI,0.708 - 0.748)。此外,DCA表明,与传统分期系统相比,列线图具有正的净效益。在训练集和验证集中,高风险组的iCCA癌症特异性死亡概率高于低风险组;同时,高风险组患者的总生存期(OS)明显低于低风险组。
老年iCCA患者与非老年iCCA患者具有相当的长期预后。此外,我们基于竞争风险分析构建了一个预测老年iCCA患者生存的预后列线图。竞争风险列线图显示出出色的鉴别能力和校准效果。