Columbia University Irving Medical Center, New York, New York.
Division of General Medicine, Department of Medicine, Columbia University Irving Medical Center, New York, New York.
JAMA Netw Open. 2020 Nov 2;3(11):e2025134. doi: 10.1001/jamanetworkopen.2020.25134.
Adults who belong to racial/ethnic minority groups are more likely than White adults to receive a diagnosis of chronic disease in the United States.
To evaluate which health indicators have improved or become worse among Black and Hispanic middle-aged and older adults since the Minority Health and Health Disparities Research and Education Act of 2000.
DESIGN, SETTING, AND PARTICIPANTS: In this repeated cross-sectional study, a total of 4 856 326 records were extracted from the Behavioral Risk Factor Surveillance System from January 1999 through December 2018 of persons who self-identified as Black (non-Hispanic), Hispanic (non-White), or White and who were 45 years or older.
The 1999 legislation to reduce racial/ethnic health disparities.
Poor health indicators and disparities including major chronic diseases, physical inactivity, uninsured status, and overall poor health.
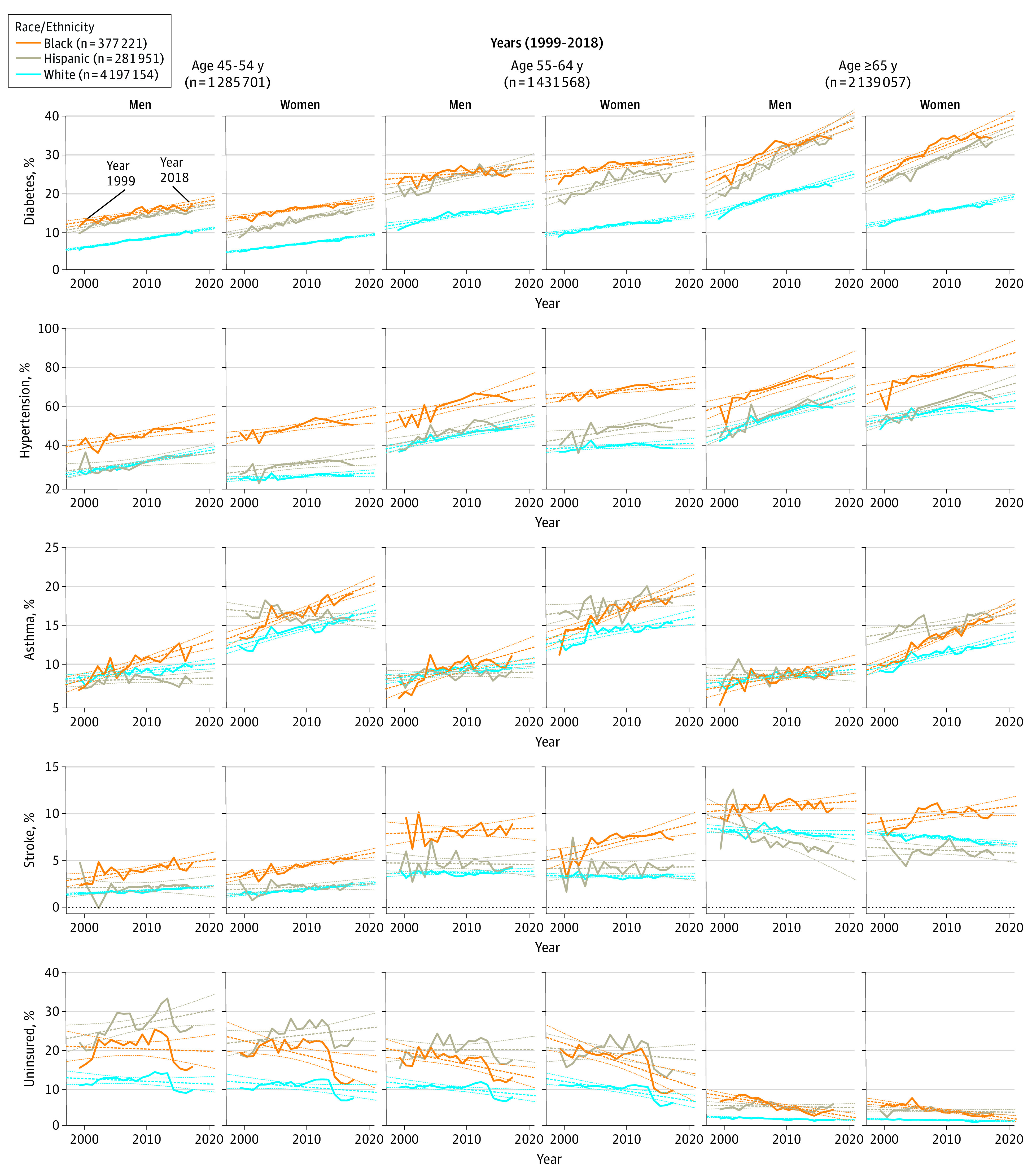
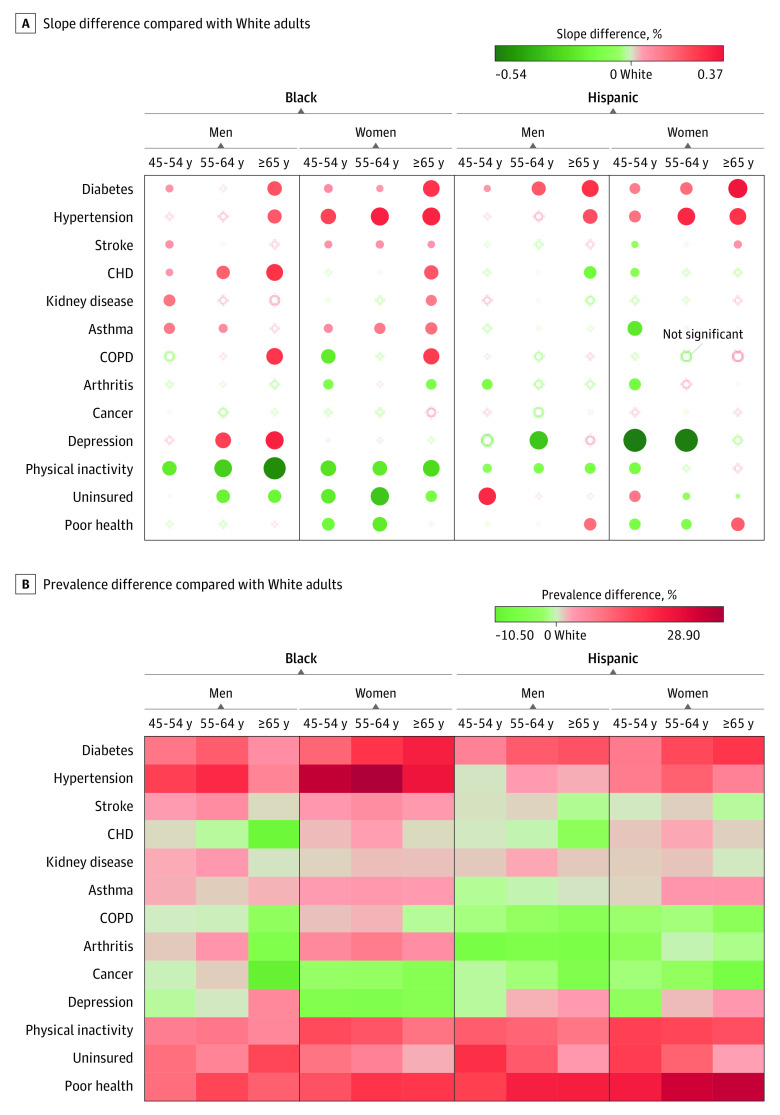
Among the 4 856 326 participants (2 958 041 [60.9%] women; mean [SD] age, 60.4 [11.8] years), Black adults showed an overall decrease indicating improvement in uninsured status (β = -0.40%; P < .001) and physical inactivity (β = -0.29%; P < .001), while they showed an overall increase indicating deterioration in hypertension (β = 0.88%; P < .001), diabetes (β = 0.52%; P < .001), asthma (β = 0.25%; P < .001), and stroke (β = 0.15%; P < .001) during the last 20 years. The Black-White gap (ie, the change in β between groups) showed improvement (2 trend lines converging) in uninsured status (-0.20%; P < .001) and physical inactivity (-0.29%; P < .001), while the Black-White gap worsened (2 trend lines diverging) in diabetes (0.14%; P < .001), hypertension (0.15%; P < .001), coronary heart disease (0.07%; P < .001), stroke (0.07%; P < .001), and asthma (0.11%; P < .001). Hispanic adults showed improvement in physical inactivity (β = -0.28%; P = .02) and perceived poor health (β = -0.22%; P = .001), while they showed overall deterioration in hypertension (β = 0.79%; P < .001) and diabetes (β = 0.50%; P < .001). The Hispanic-White gap showed improvement in coronary heart disease (-0.15%; P < .001), stroke (-0.04%; P < .001), kidney disease (-0.06%; P < .001), asthma (-0.06%; P = .02), arthritis (-0.26%; P < .001), depression (-0.23%; P < .001), and physical inactivity (-0.10%; P = .001), while the Hispanic-White gap worsened in diabetes (0.15%; P < .001), hypertension (0.05%; P = .03), and uninsured status (0.09%; P < .001).
This study suggests that Black-White disparities increased in diabetes, hypertension, and asthma, while Hispanic-White disparities remained in diabetes, hypertension, and uninsured status.
在美国,属于少数族裔的成年人比白人成年人更有可能被诊断出患有慢性疾病。
评估自 2000 年《少数民族健康和健康差异研究与教育法案》以来,黑人和西班牙裔中年及以上成年人的哪些健康指标有所改善或恶化。
设计、地点和参与者:在这项重复的横断面研究中,从 1999 年 1 月至 2018 年 12 月,从行为风险因素监测系统中提取了 4856326 条记录,这些记录来自自认为是黑人(非西班牙裔)、西班牙裔(非白人)或白人且年龄在 45 岁及以上的人群。
1999 年减少种族/族裔健康差异的立法。
包括主要慢性疾病、身体活动不足、未参保状态和整体健康状况不佳在内的不良健康指标和差异。
在 4856326 名参与者中(2958041 名[60.9%]女性;平均[SD]年龄,60.4[11.8]岁),黑人成年人的整体未参保率呈下降趋势,表明未参保状态有所改善(β=-0.40%;P<0.001),身体活动不足的比例也呈下降趋势(β=-0.29%;P<0.001),而高血压(β=0.88%;P<0.001)、糖尿病(β=0.52%;P<0.001)、哮喘(β=0.25%;P<0.001)和中风(β=0.15%;P<0.001)的整体比例则呈上升趋势,表明在过去 20 年里这些疾病有所恶化。黑人和白人之间的差距(即两组之间β的变化)在未参保状态(-0.20%;P<0.001)和身体活动不足(-0.29%;P<0.001)方面有所改善(两条趋势线趋于收敛),而在糖尿病(0.14%;P<0.001)、高血压(0.15%;P<0.001)、冠心病(0.07%;P<0.001)、中风(0.07%;P<0.001)和哮喘(0.11%;P<0.001)方面的差距则有所扩大(两条趋势线发散)。西班牙裔成年人在身体活动不足(β=-0.28%;P=0.02)和自我感知健康状况不佳(β=-0.22%;P=0.001)方面有所改善,而在高血压(β=0.79%;P<0.001)和糖尿病(β=0.50%;P<0.001)方面则整体恶化。西班牙裔和白人之间的差距在冠心病(-0.15%;P<0.001)、中风(-0.04%;P<0.001)、肾病(-0.06%;P<0.001)、哮喘(-0.06%;P=0.02)、关节炎(-0.26%;P<0.001)、抑郁症(-0.23%;P<0.001)和身体活动不足(-0.10%;P=0.001)方面有所改善,而在糖尿病(0.15%;P<0.001)、高血压(0.05%;P=0.03)和未参保状态(0.09%;P<0.001)方面的差距则有所扩大。
这项研究表明,黑人和白人之间的糖尿病、高血压和哮喘的差距在增加,而西班牙裔和白人之间的糖尿病、高血压和未参保状态的差距仍然存在。