Honeywell Richard J, Kathmann Ietje, Giovannetti Elisa, Tibaldi Carmelo, Smit Egbert F, Rovithi Maria N, Verheul Henk M W, Peters Godefridus J
Department of Medical Oncology, Amsterdam UMC, VU University Medical Center, PO Box 7057, 1007 MB Amsterdam, The Netherlands.
Department of Pharmacy, Amsterdam UMC, VU University Medical Center, PO Box 7057, 1007 MB Amsterdam, The Netherlands.
Cancers (Basel). 2020 Nov 10;12(11):3322. doi: 10.3390/cancers12113322.
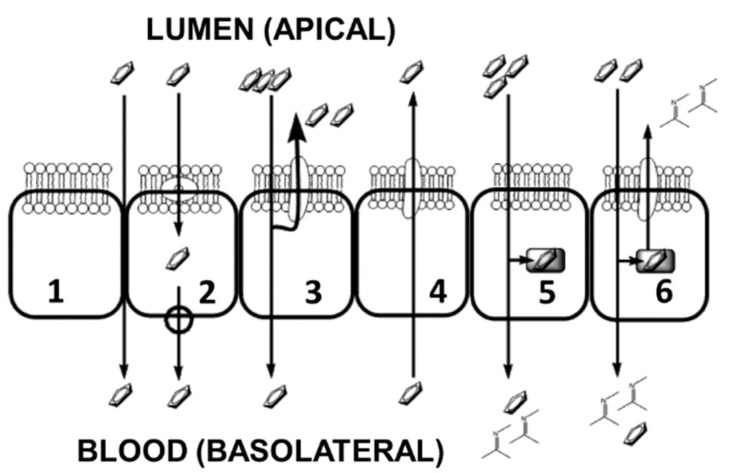
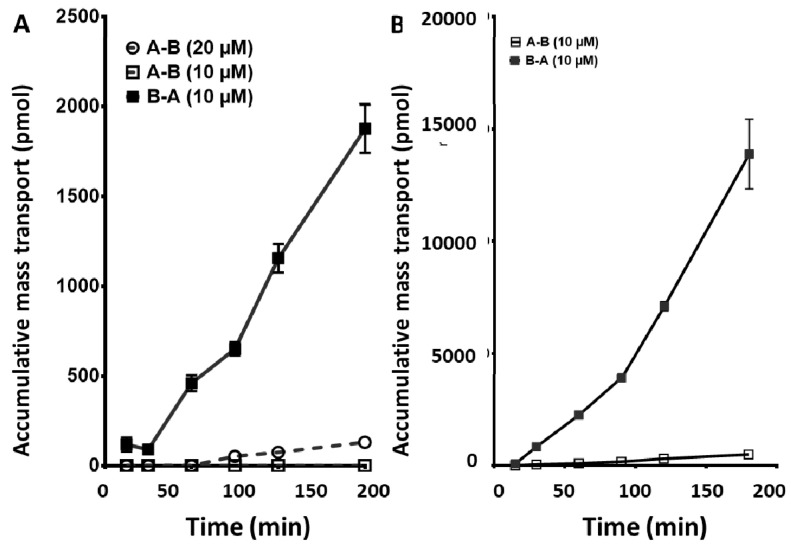
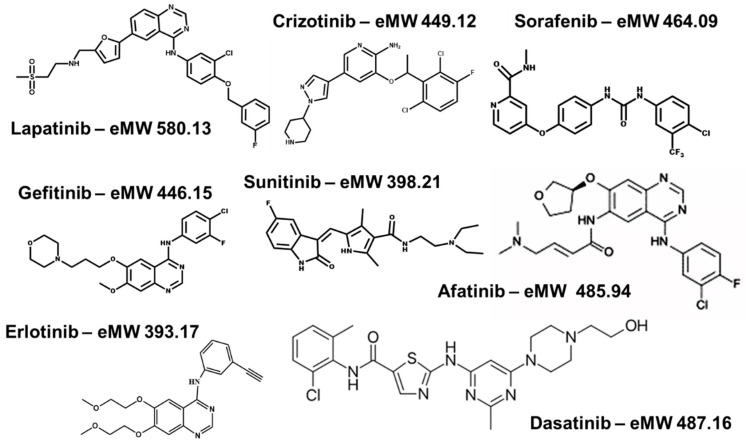
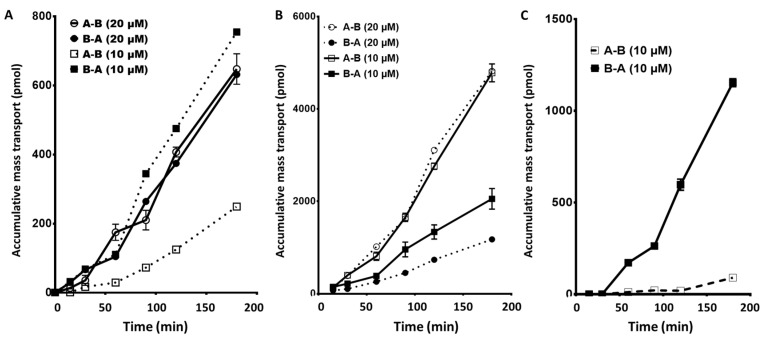
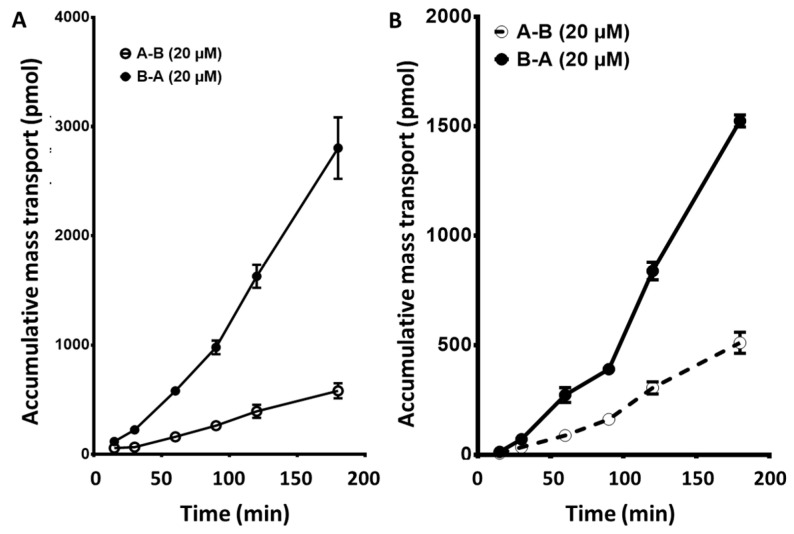
tyrosine kinase inhibitors (TKIs) inhibit phosphorylation of signaling proteins. TKIs often show large variations in the clinic due to poor pharmacology, possibly leading to resistance. We compared gut absorption of inhibitors of epidermal growth factor receptor (erlotinib, gefitinib, and afatinib), ALK-cMET (crizotinib), PDGFR/BCR-Abl (dasatinib), and multikinase inhibitors (sunitinib and sorafenib). In clinical samples, we measured the disposition of each compound within various blood compartments. we used an optimized CaCo2 gut epithelial model to characterize 20 µM TKI absorption. The apical/basolateral transfer is considered to represent the gut/blood transfer. Drugs were measured using LC-MS/MS. sorafenib and sunitinib showed the highest apical/basolateral transfer (P 14.1 and 7.7 × 10 cm/s, respectively), followed by dasatinib (3.4), afatinib (1.5), gefitinib (0.38), erlotinib (0.13), and crizotinib (n.d.). However, the net absorptions for dasatinib, afatinib, crizotinib, and erlotinib were highly negative (efflux ratios >5) or neutral/negative, sorafenib (0.86), gefitinib (1.0), and sunitinib (1.6). A high negative absorption may result in resistance because of a poor exposure of tissues to the drug. Accumulation of the TKIs at the end of the transfer period (A->B) was not detectable for erlotinib, very low for afatinib 0.45 pmol/μg protein), followed by gefitinib (0.79), dasatinib (1.1), sorafenib (1.65), and crizotinib (2.11), being highest for sunitinib (11.9). A similar pattern was found for accumulation of these drugs in other colon cell lines, WiDr and HT29. In clinical samples, drugs accumulated consistently in red blood cells; blood to plasma ratios were all > 3 (sorafenib) or over 30 for erlotinib. TKIs are consistently poorly absorbed, but accumulation in red blood cells seems to compensate for this.
酪氨酸激酶抑制剂(TKIs)可抑制信号蛋白的磷酸化。由于药理学特性不佳,TKIs在临床上常常表现出较大差异,这可能会导致耐药性。我们比较了表皮生长因子受体抑制剂(厄洛替尼、吉非替尼和阿法替尼)、ALK-cMET抑制剂(克唑替尼)、PDGFR/BCR-Abl抑制剂(达沙替尼)以及多激酶抑制剂(舒尼替尼和索拉非尼)的肠道吸收情况。在临床样本中,我们测定了每种化合物在不同血液成分中的分布情况。我们使用优化后的CaCo2肠道上皮模型来表征20µM TKIs的吸收情况。顶侧/基底侧转运被认为代表肠道/血液转运。使用液相色谱-串联质谱法(LC-MS/MS)测定药物。舒尼替尼和索拉非尼表现出最高的顶侧/基底侧转运(分别为P 14.1和7.7×10 cm/s),其次是达沙替尼(3.4)、阿法替尼(1.5)、吉非替尼(0.38)、厄洛替尼(0.13)和克唑替尼(未检测到)。然而,达沙替尼、阿法替尼、克唑替尼和厄洛替尼的净吸收为高度负值(外排率>5)或中性/负值,舒尼替尼为0.86,吉非替尼为1.0,索拉非尼为1.6。高负吸收可能会由于组织对药物的暴露不足而导致耐药性。在转运期结束时(A->B),厄洛替尼未检测到TKIs的积累,阿法替尼积累量非常低(0.45 pmol/μg蛋白),其次是吉非替尼(0.79)、达沙替尼(1.1)、索拉非尼(1.65)和克唑替尼(2.11),舒尼替尼积累量最高(11.9)。在其他结肠细胞系WiDr和HT29中,这些药物的积累也发现了类似的模式。在临床样本中,药物在红细胞中持续积累;血液与血浆的比值对于索拉非尼均>3,对于厄洛替尼则超过30。TKIs的吸收一直很差,但在红细胞中的积累似乎可以弥补这一点。