Gao Yanmei, Yang Chunhe, He Ning, Zhao Guodong, Wang Jianfei, Yang Yadong
Department of Radiotherapy, Tumor Hospital of Shaanxi Province, Affiliated to the Medical College of Xi'an Jiaotong University, Xi'an, China.
GloriousMed Clinical Laboratory (Shanghai) Co., Ltd, Shanghai, China.
Front Oncol. 2020 Oct 30;10:571545. doi: 10.3389/fonc.2020.571545. eCollection 2020.
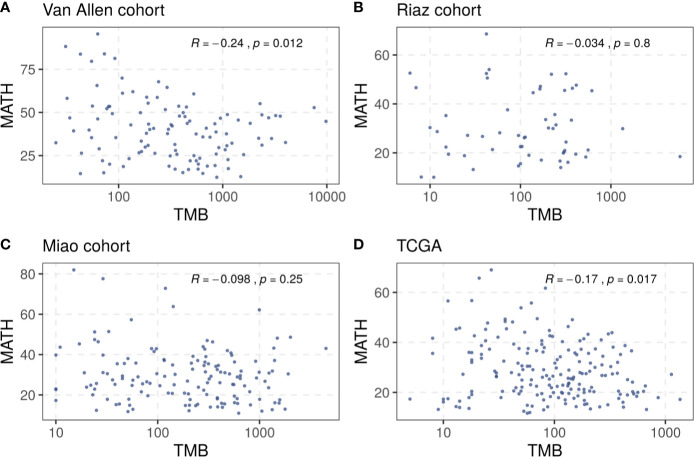
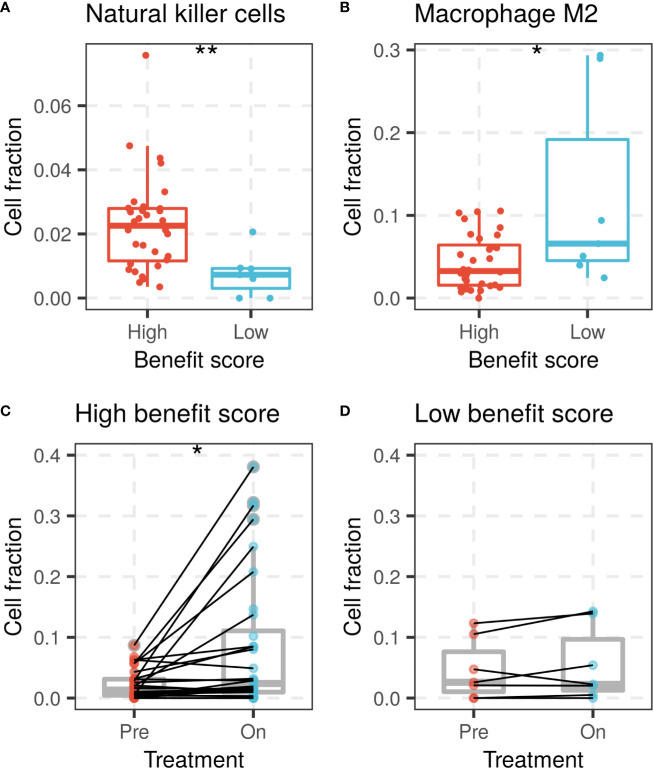
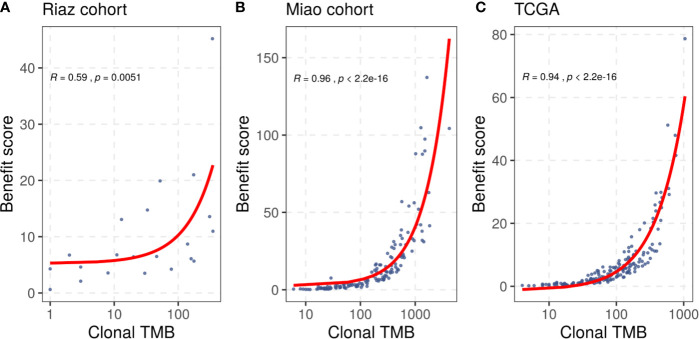
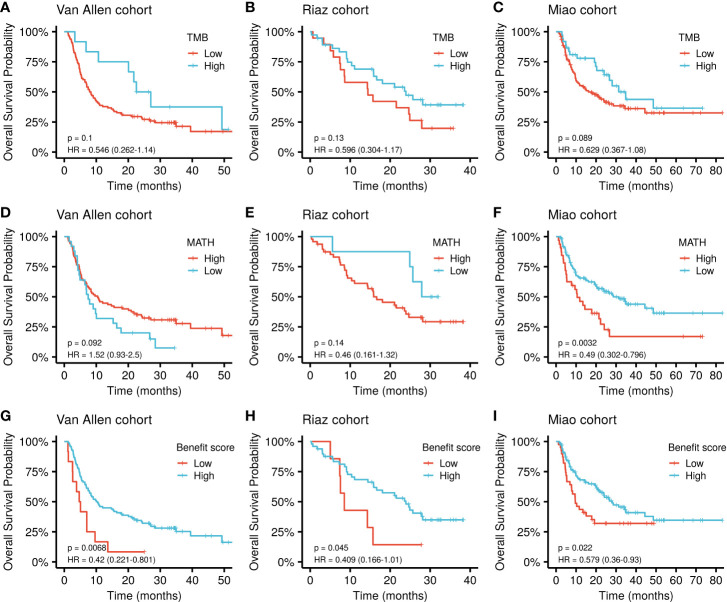
The tumor mutational burden (TMB) has been reported as a predictive marker of the response to immune checkpoint inhibition (ICI) therapy in previous melanoma clinical trials. However, the TMB alone is not sufficient to accurately predict immunotherapy benefit. Additional biomarkers are needed for better stratification of immunotherapy-sensitive patients. In the present study, mutation data and survival information of patients with melanoma were collected from several immunotherapy studies, and tumor heterogeneity was estimated using mutant-allele tumor heterogeneity (MATH). The benefit score was defined as the ratio between the TMB and tumor heterogeneity, and optimal critical values were selected to group patients and evaluate their response to ICI treatment. The benefit score significantly improved the performance of stratifying the overall survival of patients compared with the TMB alone as a predictor in two independent cohorts (p = 0.0068 . p = 0.1 and p = 0.045 . p = 0.13), in which patients were treated with Ipilimumab and Nivolumab, respectively. In another cohort of patients with melanoma receiving mixed ICI treatment, the benefit score was also positively associated with higher overall survival (p = 0.022) and outperformed the TMB alone, with a significance of p = 0.089. The benefit score showed a positive correlation with clonal TMB, a reported immunotherapy marker, and exceeded it in immunotherapy response prediction. Besides, a high benefit score was found to be associated with higher proportions of natural killer cells, lower proportions of M2 macrophages and elevated CD8 T cells, all of which favor ICI therapy. In summary, tumor heterogeneity combined with the TMB showed superior efficacy in predicting the response to ICI therapy. This might further help to delineate the mechanisms of immunotherapy in patients with melanoma.
在先前的黑色素瘤临床试验中,肿瘤突变负荷(TMB)已被报道为免疫检查点抑制(ICI)治疗反应的预测标志物。然而,仅TMB不足以准确预测免疫治疗的获益情况。需要额外的生物标志物来更好地对免疫治疗敏感患者进行分层。在本研究中,从多项免疫治疗研究中收集了黑色素瘤患者的突变数据和生存信息,并使用突变等位基因肿瘤异质性(MATH)来估计肿瘤异质性。将获益评分定义为TMB与肿瘤异质性的比值,并选择最佳临界值对患者进行分组,评估他们对ICI治疗的反应。在两个独立队列中,与单独使用TMB作为预测指标相比,获益评分显著提高了对患者总生存进行分层的性能(p = 0.0068,p = 0.1;p = 0.045,p = 0.13),这两个队列中的患者分别接受了伊匹单抗和纳武单抗治疗。在另一组接受混合ICI治疗的黑色素瘤患者中,获益评分也与较高的总生存率呈正相关(p = 0.022),并且优于单独的TMB,p值为0.089。获益评分与已报道的免疫治疗标志物克隆TMB呈正相关,并且在免疫治疗反应预测方面超过了克隆TMB。此外,发现高获益评分与较高比例的自然杀伤细胞、较低比例的M2巨噬细胞以及升高的CD8 T细胞相关,所有这些都有利于ICI治疗。总之,肿瘤异质性与TMB相结合在预测ICI治疗反应方面显示出卓越的效能。这可能进一步有助于阐明黑色素瘤患者免疫治疗的机制。