Roberts Kirsty A, Colley Liam, Agbaedeng Thomas A, Ellison-Hughes Georgina M, Ross Mark D
Research Institute for Sport and Exercise Sciences, Liverpool John Moores University, Liverpool, United Kingdom.
School of Sport, Health & Exercise Science, Bangor University, Bangor, United Kingdom.
Front Cardiovasc Med. 2020 Oct 26;7:598400. doi: 10.3389/fcvm.2020.598400. eCollection 2020.
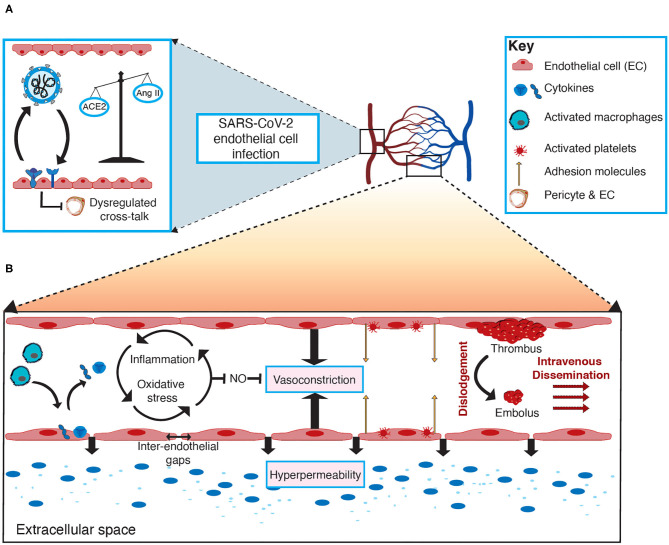
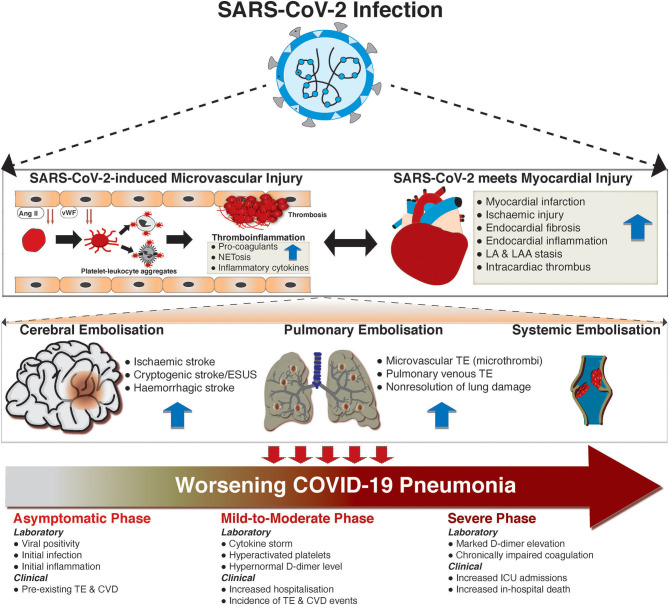
The coronavirus pandemic has reportedly infected over 31.5 million individuals and caused over 970,000 deaths worldwide (as of 22nd Sept 2020). This novel coronavirus, officially named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), although primarily causes significant respiratory distress, can have significant deleterious effects on the cardiovascular system. Severe cases of the virus frequently result in respiratory distress requiring mechanical ventilation, often seen, but not confined to, individuals with pre-existing hypertension and cardiovascular disease, potentially due to the fact that the virus can enter the circulation via the lung alveoli. Here the virus can directly infect vascular tissues, via TMPRSS2 spike glycoprotein priming, thereby facilitating ACE-2-mediated viral entry. Clinical manifestations, such as vasculitis, have been detected in a number of vascular beds (e.g., lungs, heart, and kidneys), with thromboembolism being observed in patients suffering from severe coronavirus disease (COVID-19), suggesting the virus perturbs the vasculature, leading to vascular dysfunction. Activation of endothelial cells via the immune-mediated inflammatory response and viral infection of either endothelial cells or cells involved in endothelial homeostasis, are some of the multifaceted mechanisms potentially involved in the pathogenesis of vascular dysfunction within COVID-19 patients. In this review, we examine the evidence of vascular manifestations of SARS-CoV-2, the potential mechanism(s) of entry into vascular tissue and the contribution of endothelial cell dysfunction and cellular crosstalk in this vascular tropism of SARS-CoV-2. Moreover, we discuss the current evidence on hypercoagulability and how it relates to increased microvascular thromboembolic complications in COVID-19.
据报道,新冠疫情已在全球感染了超过3150万人,并导致超过97万人死亡(截至2020年9月22日)。这种新型冠状病毒,正式名称为严重急性呼吸综合征冠状病毒2(SARS-CoV-2),虽然主要导致严重的呼吸窘迫,但也会对心血管系统产生重大有害影响。该病毒的严重病例经常导致需要机械通气的呼吸窘迫,常见于(但不限于)患有高血压和心血管疾病的患者,这可能是因为病毒可通过肺泡进入循环系统。在这里,病毒可通过跨膜丝氨酸蛋白酶2(TMPRSS2)刺突糖蛋白引发作用直接感染血管组织,从而促进血管紧张素转换酶2(ACE-2)介导的病毒进入。在多个血管床(如肺、心脏和肾脏)中已检测到血管炎等临床表现,在患有严重冠状病毒病(COVID-19)的患者中观察到血栓栓塞,这表明该病毒扰乱了脉管系统,导致血管功能障碍。通过免疫介导的炎症反应激活内皮细胞以及内皮细胞或参与内皮稳态的细胞受到病毒感染,是可能参与COVID-19患者血管功能障碍发病机制的一些多方面机制。在这篇综述中,我们研究了SARS-CoV-2血管表现的证据、进入血管组织的潜在机制以及内皮细胞功能障碍和细胞间相互作用在SARS-CoV-2这种血管嗜性中的作用。此外,我们讨论了目前关于高凝状态的证据以及它与COVID-19中微血管血栓栓塞并发症增加的关系。