Department of Cardiovascular Medicine, Heart, Vascular and Thoracic Institute, Cleveland Clinic, Cleveland, Ohio.
Department of Cardiovascular Medicine, Heart, Vascular and Thoracic Institute, Cleveland Clinic, Cleveland, Ohio.
Am J Cardiol. 2021 Feb 15;141:140-146. doi: 10.1016/j.amjcard.2020.11.009. Epub 2020 Nov 18.
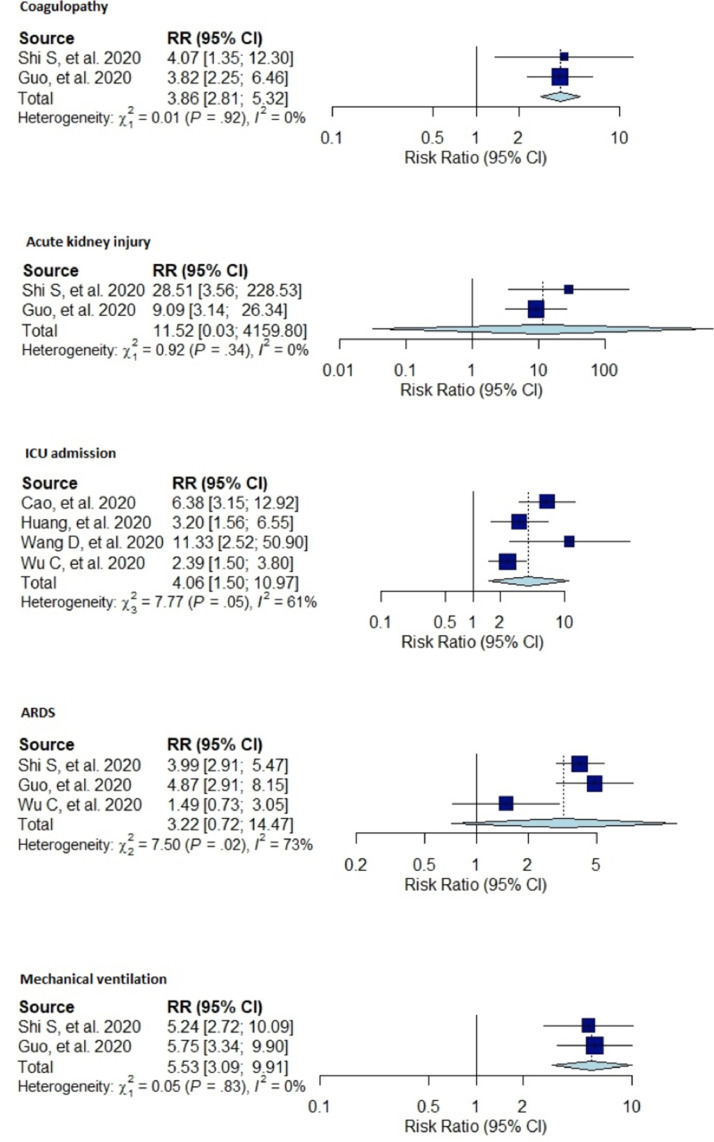
Current evidence is limited to small studies describing the association between cardiac injury and outcomes in patients with coronavirus disease 2019 (COVID-19). To address this, we performed a comprehensive meta-analysis of studies in COVID-19 patients to evaluate the association between cardiac injury and all-cause mortality, intensive care unit (ICU) admission, mechanical ventilation, acute respiratory distress syndrome, acute kidney injury and coagulopathy. Further, studies comparing cardiac biomarker levels in survivors versus nonsurvivors were included. A total of 14 studies (3,175 patients) were utilized for the final analysis. Cardiac injury in patients with COVID-19 was associated with higher risk of mortality (risk ratio [RR]:7.79; 95% confidence interval [CI]: 4.69 to 13.01; I=58%), ICU admission (RR: 4.06; 95% CI: 1.50 to 10.97; I = 61%), mechanical ventilation (RR: 5.53; 95% CI: 3.09 to 9.91; I = 0%), and developing coagulopathy (RR: 3.86; 95% CI:2.81 to 5.32; I = 0%). However, cardiac injury was not associated with increased risk of acute respiratory distress syndrome (RR:3.22; 95% CI:0.72 to 14.47; I = 73%) or acute kidney injury (RR: 11.52, 95% CI:0.03 to 4,159.80; I = 0%). The levels of hs-cTnI (MD:34.54 pg/ml;95% CI: 24.67 to 44.40 pg/ml; I = 88%), myoglobin (MD:186.81 ng/ml; 95% CI: 121.52 to 252.10 ng/ml; I = 88%), NT-pro BNP (MD:1183.55 pg/ml; 95% CI: 520.19 to 1846.91 pg/ml: I = 96%) and CK-MB (MD:2.49 ng/ml;95% CI: 1.86 to 3.12 ng/ml; I = 90%) were significantly elevated in nonsurvivors compared with survivors with COVID-19 infection. The results of this meta-analysis suggest that cardiac injury is associated with higher mortality, ICU admission, mechanical ventilation and coagulopathy in patients with COVID-19.
目前的证据仅限于描述 COVID-19 患者中心脏损伤与结局之间关联的小型研究。为了解决这一问题,我们对 COVID-19 患者的研究进行了全面的荟萃分析,以评估心脏损伤与全因死亡率、重症监护病房(ICU)入院、机械通气、急性呼吸窘迫综合征、急性肾损伤和凝血障碍之间的关联。此外,还纳入了比较 COVID-19 幸存者和非幸存者心脏生物标志物水平的研究。最终分析共纳入了 14 项研究(3175 例患者)。COVID-19 患者的心脏损伤与更高的死亡率风险相关(风险比 [RR]:7.79;95%置信区间 [CI]:4.69 至 13.01;I=58%)、ICU 入院(RR:4.06;95%CI:1.50 至 10.97;I=61%)、机械通气(RR:5.53;95%CI:3.09 至 9.91;I=0%)和凝血障碍(RR:3.86;95%CI:2.81 至 5.32;I=0%)。然而,心脏损伤与急性呼吸窘迫综合征(RR:3.22;95%CI:0.72 至 14.47;I=73%)或急性肾损伤(RR:11.52,95%CI:0.03 至 4159.80;I=0%)风险增加无关。hs-cTnI(MD:34.54pg/ml;95%CI:24.67 至 44.40pg/ml;I=88%)、肌红蛋白(MD:186.81ng/ml;95%CI:121.52 至 252.10ng/ml;I=88%)、NT-proBNP(MD:1183.55pg/ml;95%CI:520.19 至 1846.91pg/ml;I=96%)和 CK-MB(MD:2.49ng/ml;95%CI:1.86 至 3.12ng/ml;I=90%)的水平在 COVID-19 感染的非幸存者中明显高于幸存者。这项荟萃分析的结果表明,心脏损伤与 COVID-19 患者的死亡率、ICU 入院、机械通气和凝血障碍升高有关。