Intensive Care Unit Peking University Shougang Hospital, Beijing, China.
Department of Emergency, Peking University People's Hospital, Beijing, China.
BMC Nephrol. 2020 Nov 23;21(1):499. doi: 10.1186/s12882-020-02119-7.
TAFRO syndrome is a clinical subtype of idiopathic multicentric Castleman disease (iMCD) that is characterized by thrombocytopenia, anasarca, fever, reticulin myelofibrosis (or renal dysfunction), and organomegaly. TAFRO syndrome has only recently been described, and many clinicians are unaware of this disease, leading to delays in diagnosis and treatment. We present two patients with TAFRO syndrome in whom renal biopsies were performed.
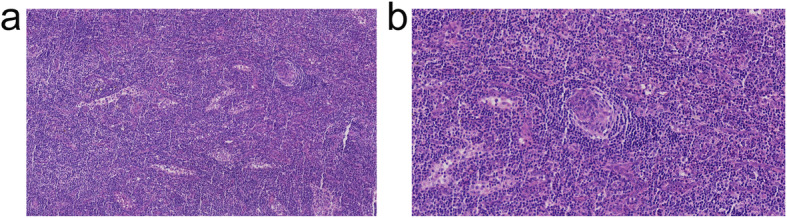
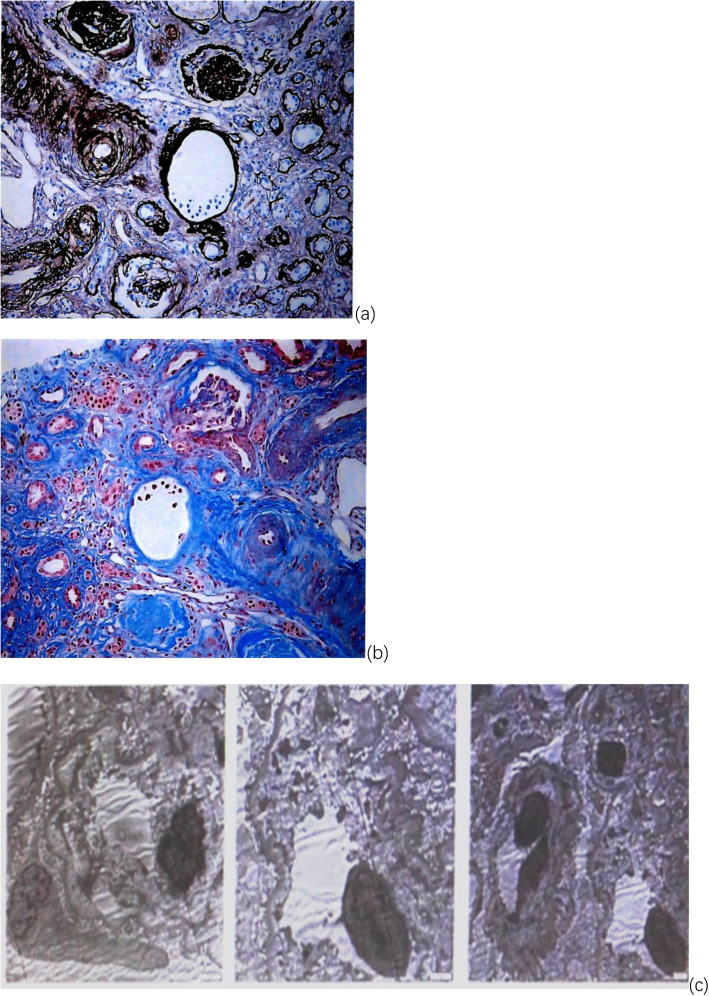
Both patients had subacute onset and exhibited renal insufficiency, edema, anemia, thrombocytopenia, polyserositis and lymphadenopathy over the disease course. However, there were many differences in their clinical manifestations. Case 1 was a 30-year-old woman admitted due to intermittent vaginal bleeding for 3 weeks. Laboratory tests on admission showed severe renal insufficiency (creatinine: 624 μmol/L), severe anemia (Hb: 41 g/L), and moderate thrombocytopenia (61 × 10/L). Case 2 was a 42-year-old man. Acute epigastric pain was his initial complaint, and computed tomography (CT) revealed retroperitoneal exudation around the pancreas. He was diagnosed with acute pancreatitis, and after treatment with a proton pump inhibitor (PPI) and somatostatin, his abdominal pain still recurred. During treatment, renal failure gradually increased, with oliguria, fever, anemia, thrombocytopenia, edema and massive ascites. Lymph node histologies were consistent with the hyaline-vascular (HV) type and mixed type, respectively, and renal histopathologies were consistent with thrombotic microangiopathy (TMA)-like renal lesions and membranoproliferative glomerulonephritis (MPGN), respectively. Their general conditions improved after glucocorticoid therapy, but their renal functions did not recover completely. On the basis of glucocorticoids, second-line treatments with tocilizumab and rituximab, respectively, were applied.
The diagnosis of TAFRO syndrome is based mainly on clinical manifestations and lymph node biopsies. A reliable early diagnosis and appropriate rapid treatment are essential to improve patient outcomes. Clinicians should deepen their understanding of this disease and similar conditions. Once the disease is suspected, lymph node biopsies should be performed as soon as possible. In addition, renal biopsies should be actively performed in patients with renal involvement.
TAFRO 综合征是特发性多中心 Castleman 病(iMCD)的一种临床亚型,其特征为血小板减少症、全身性水肿、发热、网状纤维性骨髓纤维化(或肾功能障碍)和器官肿大。TAFRO 综合征最近才被描述,许多临床医生对此病并不了解,导致诊断和治疗延误。我们报告了两名接受肾活检的 TAFRO 综合征患者。
两名患者均为亚急性起病,在疾病过程中表现为肾功能不全、水肿、贫血、血小板减少、多浆膜炎和淋巴结病。然而,他们的临床表现存在许多差异。病例 1 为 30 岁女性,因阴道间断出血 3 周入院。入院时实验室检查显示严重肾功能不全(肌酐:624 μmol/L)、严重贫血(Hb:41 g/L)和中度血小板减少症(61×10/L)。病例 2 为 42 岁男性,首发症状为急性上腹痛,CT 显示胰腺周围腹膜后渗出。他被诊断为急性胰腺炎,质子泵抑制剂(PPI)和生长抑素治疗后腹痛仍反复发作。在治疗过程中,肾功能逐渐恶化,出现少尿、发热、贫血、血小板减少、水肿和大量腹水。淋巴结组织学检查分别符合透明血管(HV)型和混合型,肾组织学检查分别符合血栓性微血管病(TMA)样肾病变和膜增生性肾小球肾炎(MPGN)。糖皮质激素治疗后一般情况改善,但肾功能未完全恢复。在此基础上,分别应用托珠单抗和利妥昔单抗二线治疗。
TAFRO 综合征的诊断主要基于临床表现和淋巴结活检。可靠的早期诊断和适当的快速治疗对于改善患者预后至关重要。临床医生应加深对该病和类似疾病的认识。一旦怀疑该病,应尽快进行淋巴结活检。此外,对于有肾脏受累的患者,应积极进行肾活检。