Naganawa Mika, Gallezot Jean-Dominique, Shah Vijay, Mulnix Tim, Young Colin, Dias Mark, Chen Ming-Kai, Smith Anne M, Carson Richard E
PET Center, Department of Radiology and Biomedical Imaging, Yale University, New Haven, CT, USA.
Molecular Imaging, Siemens Medical Solutions USA, Inc., Knoxville, TN, USA.
EJNMMI Phys. 2020 Nov 23;7(1):67. doi: 10.1186/s40658-020-00330-x.
Arterial blood sampling is the gold standard method to obtain the arterial input function (AIF) for quantification of whole body (WB) dynamic F-FDG PET imaging. However, this procedure is invasive and not typically available in clinical environments. As an alternative, we compared AIFs to population-based input functions (PBIFs) using two normalization methods: area under the curve (AUC) and extrapolated initial plasma concentration (C*(0)). To scale the PBIFs, we tested two methods: (1) the AUC of the image-derived input function (IDIF) and (2) the estimated C*(0). The aim of this study was to validate IDIF and PBIF for FDG oncological WB PET studies by comparing to the gold standard arterial blood sampling.
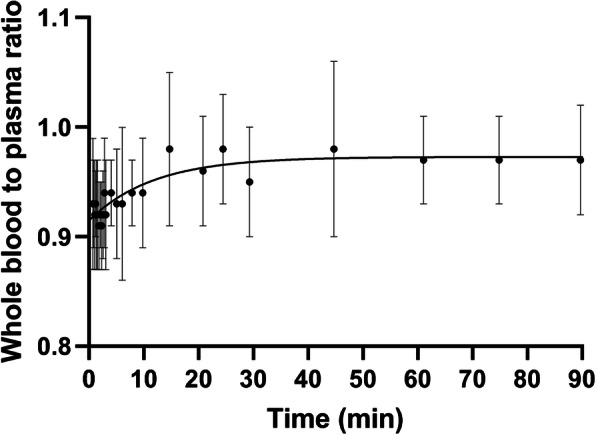
The Feng F-FDG plasma concentration model was applied to estimate AIF parameters (n = 23). AIF normalization used either AUC(0-60 min) or C*(0), estimated from an exponential fit. C*(0) is also described as the ratio of the injected dose (ID) to initial distribution volume (iDV). iDV was modeled using the subject height and weight, with coefficients that were estimated in 23 subjects. In 12 oncological patients, we computed IDIF (from the aorta) and PBIFs with scaling by the AUC of the IDIF from 4 time windows (15-45, 30-60, 45-75, 60-90 min) (PBIF) and estimated C*(0) (PBIF). The IDIF and PBIFs were compared with the gold standard AIF, using AUC values and Patlak K values.
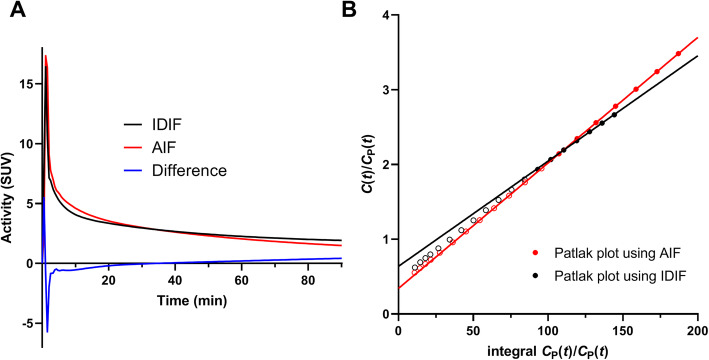
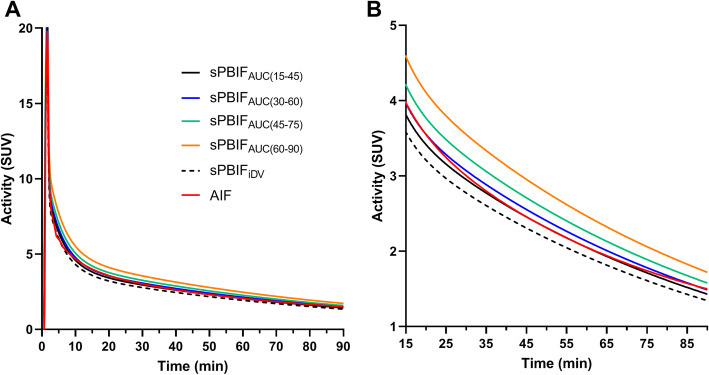
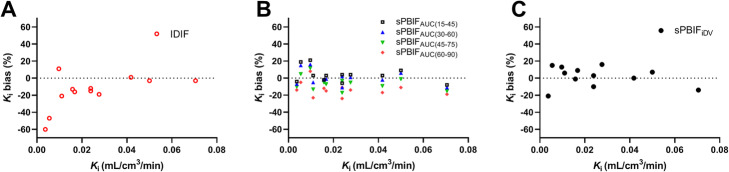
The IDIF underestimated the AIF at early times and overestimated it at later times. Thus, based on the AUC and K comparison, 30-60 min was the most accurate time window for PBIF; later time windows for scaling underestimated K (- 6 ± 8 to - 13 ± 9%). Correlations of AUC between AIF and IDIF, PBIF, and PBIF were 0.91, 0.94, and 0.90, respectively. The bias of K was - 9 ± 10%, - 1 ± 8%, and 3 ± 9%, respectively.
Both PBIF scaling methods provided good mean performance with moderate variation. Improved performance can be obtained by refining IDIF methods and by evaluating PBIFs with test-retest data.
动脉血采样是获取动脉输入函数(AIF)以对全身(WB)动态F-FDG PET成像进行定量分析的金标准方法。然而,该操作具有侵入性,且在临床环境中通常不可行。作为替代方法,我们使用两种归一化方法:曲线下面积(AUC)和外推初始血浆浓度(C*(0)),将AIF与基于人群的输入函数(PBIF)进行比较。为了对PBIF进行缩放,我们测试了两种方法:(1)图像衍生输入函数(IDIF)的AUC;(2)估计的C*(0)。本研究的目的是通过与金标准动脉血采样进行比较,验证IDIF和PBIF在FDG肿瘤学WB PET研究中的有效性。
应用冯F-FDG血浆浓度模型估计AIF参数(n = 23)。AIF归一化使用AUC(0-60分钟)或通过指数拟合估计的C*(0)。C*(0)也被描述为注射剂量(ID)与初始分布容积(iDV)的比值。iDV使用受试者身高和体重进行建模,其系数在23名受试者中进行估计。在12名肿瘤患者中,我们计算了IDIF(来自主动脉)和通过4个时间窗(15-45、30-60、45-75、60-90分钟)的IDIF的AUC进行缩放的PBIF(PBIF)以及估计的C*(0)(PBIF)。使用AUC值和Patlak K值将IDIF和PBIF与金标准AIF进行比较。
IDIF在早期低估了AIF,在后期高估了AIF。因此,基于AUC和K的比较,30-60分钟是PBIF最准确的时间窗;后期用于缩放的时间窗低估了K(-6±8%至-13±9%)。AIF与IDIF、PBIF和PBIF之间的AUC相关性分别为0.91、0.94和0.90。K的偏差分别为-9±10%、-1±8%和3±9%。
两种PBIF缩放方法均提供了良好的平均性能,且变化适中。通过改进IDIF方法以及使用重测数据评估PBIF,可以获得更好的性能。