Huang Zhiwei, Zhang Hongliang, Wang Man, Yang Weixian, Qiao Shubin, Hu Fenghuan
Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100037, China.
Rheumatol Ther. 2021 Mar;8(1):119-133. doi: 10.1007/s40744-020-00251-2. Epub 2020 Nov 23.
Treatment strategies to improve clinical outcomes in Takayasu's arteritis (TA) with coronary lesions have ranged from pharmacological therapy to invasive procedures, such as coronary angioplasty, stenting, and surgery. However, the therapeutic strategy for this kind of patient is still unclear. This study aimed to investigate the clinical characteristics and influence of revascularization versus medical therapy in TA patients with coronary artery involvement.
We analyzed the medical records of 806 TA patients between January 2008 and December 2019. Clinical features and treatment were analyzed, and patients were categorized into medical treatment and revascularization. Additionally, patients were sorted as percutaneous coronary intervention (PCI) and coronary artery bypass surgery (CABG) based on the strategy of revascularization.
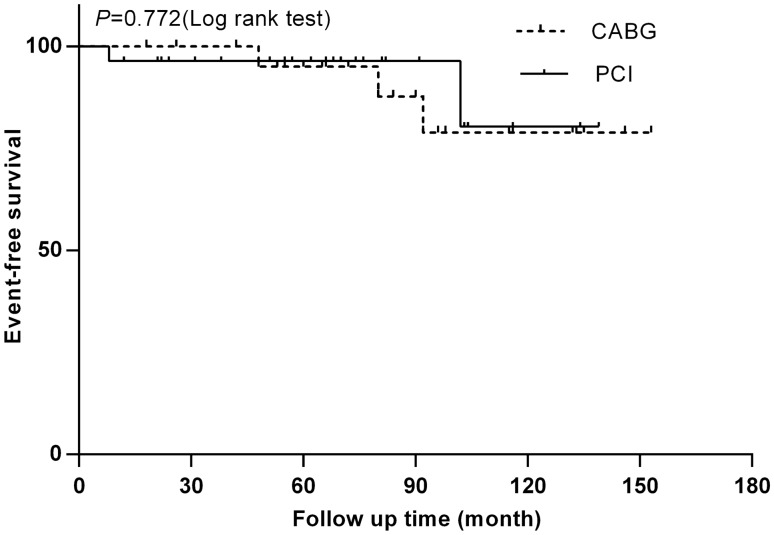
Ninety cases with coronary lesions induced by TA were enrolled. Among 90 cases, 39 patients adopted conservative treatment, and 51 patients received revascularization (28 subjects with PCI, 23 participants with CABG). The median follow-up time was 63 (45-91) months. There is no significant difference in cardiovascular death between medical treatment and revascularization (2/39, 5.1% vs. 5/51, 9.8%, P = 0.971). The analysis of subgroup indicated that the mortality caused by cardiovascular disease was also similar in the CABG and PCI (2/28, 7.1% vs. 3/23, 13.0%, P = 0.772). However, the proportion of restenosis is much higher in the PCI compared with that of CABG (39.3%, 8.7%, P = 0.022, respectively). Heart failure is an independent predictor of death in these patients.
There is no significant difference in cardiovascular death between medical treatment and revascularization. The analysis of the subgroup indicated that the mortality caused by cardiovascular disease was also similar in the CABG and PCI, but the restenosis is much higher in the PCI compared with that of CABG. Heart failure is an independent predictor of death in these patients.
改善伴有冠状动脉病变的高安动脉炎(TA)临床结局的治疗策略涵盖了从药物治疗到侵入性手术,如冠状动脉血管成形术、支架置入术和外科手术。然而,这类患者的治疗策略仍不明确。本研究旨在调查TA合并冠状动脉受累患者的临床特征以及血运重建与药物治疗的影响。
我们分析了2008年1月至2019年12月期间806例TA患者的病历。分析了临床特征和治疗情况,并将患者分为药物治疗组和血运重建组。此外,根据血运重建策略,将患者分为经皮冠状动脉介入治疗(PCI)组和冠状动脉旁路移植术(CABG)组。
纳入90例由TA引起冠状动脉病变的患者。在90例患者中,39例采用保守治疗,51例接受血运重建(28例行PCI,23例行CABG)。中位随访时间为63(45 - 91)个月。药物治疗和血运重建在心血管死亡方面无显著差异(2/39,5.1%对5/51,9.8%,P = 0.971)。亚组分析表明,CABG组和PCI组心血管疾病导致的死亡率也相似(2/28,7.1%对3/23,13.0%,P = 0.772)。然而,PCI组的再狭窄比例远高于CABG组(分别为39.3%和8.7%,P = 0.022)。心力衰竭是这些患者死亡的独立预测因素。
药物治疗和血运重建在心血管死亡方面无显著差异。亚组分析表明,CABG组和PCI组心血管疾病导致的死亡率也相似,但PCI组的再狭窄比例远高于CABG组。心力衰竭是这些患者死亡的独立预测因素。