Stone Philip W, Hickman Katherine, Steiner Michael C, Roberts C Michael, Quint Jennifer K, Singh Sally J
National Heart and Lung Institute, Imperial College London, London, UK.
West Yorkshire and Harrogate Health and Care Partnership, Bradford, Yorkshire, UK.
Int J Chron Obstruct Pulmon Dis. 2020 Nov 16;15:2941-2952. doi: 10.2147/COPD.S273336. eCollection 2020.
A large proportion of people with COPD are not referred to pulmonary rehabilitation (PR) despite its proven benefits. No previous studies have examined predictors of referral to PR.
To determine the characteristics of people with COPD associated with referral to PR.
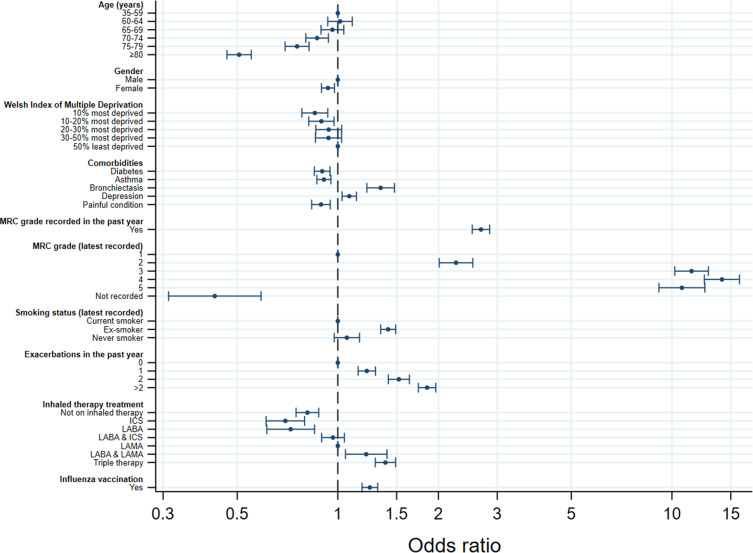
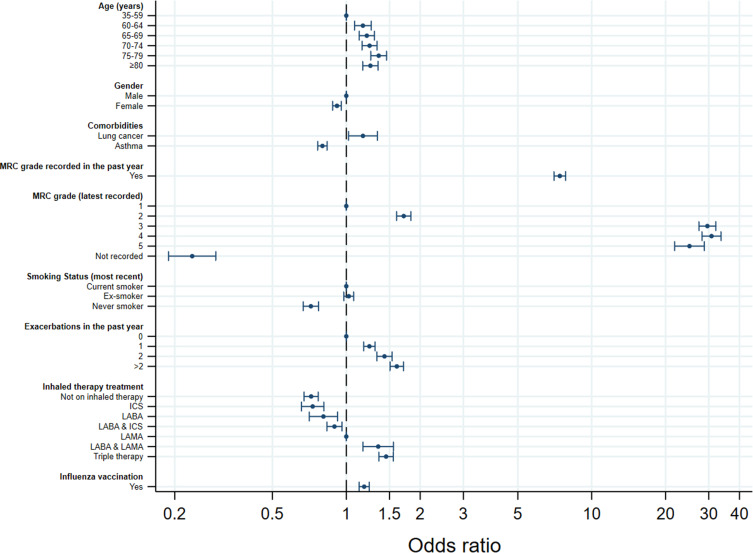
Cross-sectional analysis of a primary care cohort of 82,696 Welsh people with COPD generated as part of a UK national audit of COPD care. Data represent care received by patients as of 31/03/2017. Referral to PR was defined as any code in the patient record indicating referral to PR in the last 3 years. Potential predictors of referral to PR were chosen based on clinical judgement and data availability. Independent predictors of PR referral were determined using backward stepwise mixed-effects logistic regression with a random effect for practice. Variables assessed were: age, gender, deprivation, MRC recorded in past year, MRC grade, smoking status recorded in past year, smoking status, number of exacerbations in past year, inhaled therapy prescription, influenza vaccination, and comorbidities of diabetes, hypertension, coronary heart disease, stroke, heart failure, lung cancer, asthma, bronchiectasis, depression, anxiety, severe mental illness, osteoporosis, and painful condition.
A total of 13,297 people (16%) with COPD were referred from primary care for PR. Patients with a comorbidity of bronchiectasis or depression, MRC recorded in the last year, higher MRC grade, more exacerbations in the last year, a greater level of inhaled therapy, an influenza vaccination, or were an ex-smoker had significantly higher odds of referral to PR. Patients that were older, female, more deprived, or had a comorbidity of diabetes, asthma, or painful condition had significantly lower odds of referral to PR.
Generally appropriate patients are being prioritised for PR referral; however, it is concerning that women, current smokers, and more deprived patients appear to have lower odds of referral.
尽管肺康复(PR)已被证明有益,但很大一部分慢性阻塞性肺疾病(COPD)患者并未接受PR治疗。此前尚无研究探讨PR转诊的预测因素。
确定与PR转诊相关的COPD患者特征。
对82696名威尔士COPD患者的初级保健队列进行横断面分析,该队列是英国COPD护理全国审计的一部分。数据代表截至2017年3月31日患者接受的护理情况。PR转诊定义为患者病历中任何表明在过去3年中转诊至PR的代码。基于临床判断和数据可用性选择PR转诊的潜在预测因素。使用向后逐步混合效应逻辑回归确定PR转诊的独立预测因素,并对实践进行随机效应分析。评估的变量包括:年龄、性别、贫困程度、过去一年记录的医学研究委员会(MRC)分级、MRC等级、过去一年记录的吸烟状况、吸烟状况、过去一年的急性加重次数、吸入治疗处方、流感疫苗接种,以及糖尿病、高血压、冠心病、中风、心力衰竭、肺癌、哮喘、支气管扩张、抑郁症、焦虑症、严重精神疾病、骨质疏松症和疼痛性疾病的合并症。
共有13297名(16%)COPD患者从初级保健机构转诊接受PR治疗。合并支气管扩张或抑郁症、过去一年记录的MRC分级、较高的MRC等级、过去一年更多的急性加重次数、更高水平的吸入治疗、流感疫苗接种或已戒烟的患者转诊至PR的几率显著更高。年龄较大、女性、贫困程度较高或合并糖尿病、哮喘或疼痛性疾病的患者转诊至PR的几率显著较低。
一般来说,合适的患者被优先考虑进行PR转诊;然而,令人担忧的是,女性、当前吸烟者和贫困程度较高的患者转诊几率似乎较低。