Division of Vascular and Endovascular Surgery, Department of Surgery, University of Ottawa and The Ottawa Hospital, Ottawa, ON, Canada.
Department of Critical Care Medicine and O'Brien Institute for Public Health University of Calgary, Foothills Medical Centre, Calgary, AB, Canada.
BMJ. 2020 Nov 25;371:m4104. doi: 10.1136/bmj.m4104.
To examine the associations between neuraxial anaesthesia or general anaesthesia and clinical outcomes, length of hospital stay, and readmission in adults undergoing lower limb revascularisation surgery.
Comparative effectiveness study using linked, validated, population based databases.
Ontario, Canada, 1 April 2002 to 31 March 2015.
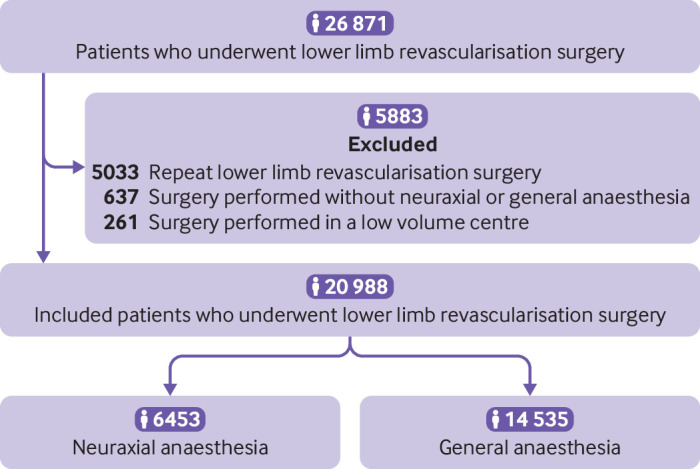
20 988 patients Ontario residents aged 18 years or older who underwent their first lower limb revascularisation surgery in hospitals performing 50 or more of these surgeries annually.
Primary outcome was 30 day all cause mortality. Secondary outcomes were in-hospital cardiopulmonary and renal complications, length of hospital stay, and 30 day readmissions. Multivariable, mixed effects regression models, adjusting for patient, procedural, and hospital characteristics, were used to estimate associations between anaesthetic technique and outcomes. Robustness of analyses were evaluated by conducting instrumental variable, propensity score matched, and survival sensitivity analyses.
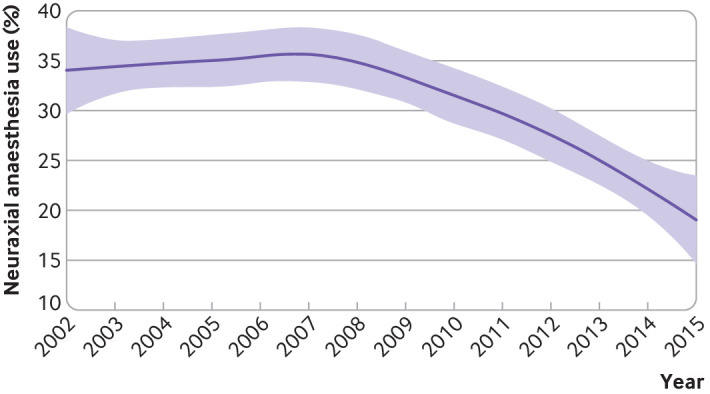
Of 20 988 patients who underwent lower limb revascularisation surgery, 6453 (30.7%) received neuraxial anaesthesia and 14 535 (69.3%) received general anaesthesia. The percentage of neuraxial anaesthesia use ranged from 0.6% to 90.6% across included hospitals. Furthermore, use of neuraxial anaesthesia declined by 17% over the study period. Death within 30 days occurred in 204 (3.2%) patients who received neuraxial anaesthesia and 646 (4.4%) patients who received general anaesthesia. After multivariable, multilevel adjustment, use of neuraxial anaesthesia compared with use of general anaesthesia was associated with decreased 30 day mortality (absolute risk reduction 0.72%, 95% confidence interval 0.65% to 0.79%; odds ratio 0.68, 95% confidence interval 0.57 to 0.83; number needed to treat to prevent one death=139). A similar direction and magnitude of association was found in instrumental variable, propensity score matched, and survival analyses. Use of neuraxial anaesthesia compared with use of general anaesthesia was also associated with decreased in-hospital cardiopulmonary and renal complications (odds ratio 0.73, 0.63 to 0.85) and a reduced length of hospital stay (-0.5 days, -0.3 to-0.6 days).
Use of neuraxial anaesthesia compared with general anaesthesia for lower limb revascularisation surgery was associated with decreased 30 day mortality and hospital length of stay. These findings might have been related to reduced cardiopulmonary and renal complications after neuraxial anaesthesia and support the increased use of neuraxial anaesthesia in patients undergoing these surgeries until the results of a large, confirmatory randomised trial become available.
探讨全身麻醉与椎管内麻醉对行下肢血运重建术成年人的临床结局、住院时间和再入院的影响。
使用已链接、验证的基于人群的数据库进行比较效果研究。
加拿大安大略省,2002 年 4 月 1 日至 2015 年 3 月 31 日。
20988 名安大略省年龄在 18 岁或以上的居民,他们在每年进行 50 次或以上此类手术的医院中首次接受下肢血运重建手术。
主要结局为 30 天全因死亡率。次要结局为住院期间心肺和肾脏并发症、住院时间和 30 天再入院率。使用多变量混合效应回归模型,根据患者、手术和医院特征进行调整,估计麻醉技术与结局之间的关联。通过进行工具变量、倾向评分匹配和生存敏感性分析来评估分析的稳健性。
在接受下肢血运重建手术的 20988 名患者中,6453 名(30.7%)接受了椎管内麻醉,14535 名(69.3%)接受了全身麻醉。在纳入的医院中,椎管内麻醉使用率从 0.6%到 90.6%不等。此外,研究期间椎管内麻醉使用率下降了 17%。接受椎管内麻醉的患者中有 204 名(3.2%)和接受全身麻醉的患者中有 646 名(4.4%)在 30 天内死亡。经过多变量、多层次调整后,与全身麻醉相比,使用椎管内麻醉与降低 30 天死亡率相关(绝对风险降低 0.72%,95%置信区间 0.65%至 0.79%;优势比 0.68,95%置信区间 0.57 至 0.83;预防一例死亡所需的人数=139)。在工具变量、倾向评分匹配和生存分析中也发现了类似的方向和程度的关联。与全身麻醉相比,使用椎管内麻醉还与住院期间心肺和肾脏并发症减少相关(优势比 0.73,0.63 至 0.85),住院时间缩短(-0.5 天,-0.3 至-0.6 天)。
与全身麻醉相比,下肢血运重建术中使用椎管内麻醉与 30 天死亡率和住院时间降低相关。这些发现可能与椎管内麻醉后心肺和肾脏并发症减少有关,并支持在这些手术中增加使用椎管内麻醉,直到一项大型确认性随机试验的结果公布。