Wellejus Albertsen Lisbeth, Heide-Jørgensen Uffe, Schmidt Sigrun Alba Johannesdottir, Grey Corina, Jackson Rod, Sørensen Henrik Toft, Schmidt Morten
Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark.
Section of Epidemiology and Biostatistics, School of Population Health, University of Auckland, Auckland, New Zealand.
Clin Epidemiol. 2020 Nov 20;12:1299-1311. doi: 10.2147/CLEP.S277325. eCollection 2020.
To develop and validate the DANish Comorbidity index for Acute Myocardial Infarction (DANCAMI) for adjustment of comorbidity burden in studies of myocardial infarction prognosis.
Using medical registries, we identified patients with first-time myocardial infarction in Denmark during 2000-2013 (n=36,685). We developed comorbidity indices predicting 1-year all-cause mortality from all comorbidities (DANCAMI) and restricted to non-cardiovascular comorbidities (rDANCAMI). For variable selection, we eliminated comorbidities stepwise using hazard ratios from multivariable Cox models. We compared DANCAMI/rDANCAMI with Charlson and Elixhauser comorbidity indices using standard performance measures (Nagelkerke's R, Harrell's C-statistic, the Integrated Discrimination Improvement, and the continuous Net Reclassification Index). We assessed the significance of the novel DANCAMI variables not included in the Charlson Comorbidity Index. External validation was performed in patients with myocardial infarction in New Zealand during 2007-2016 (n=75,069).
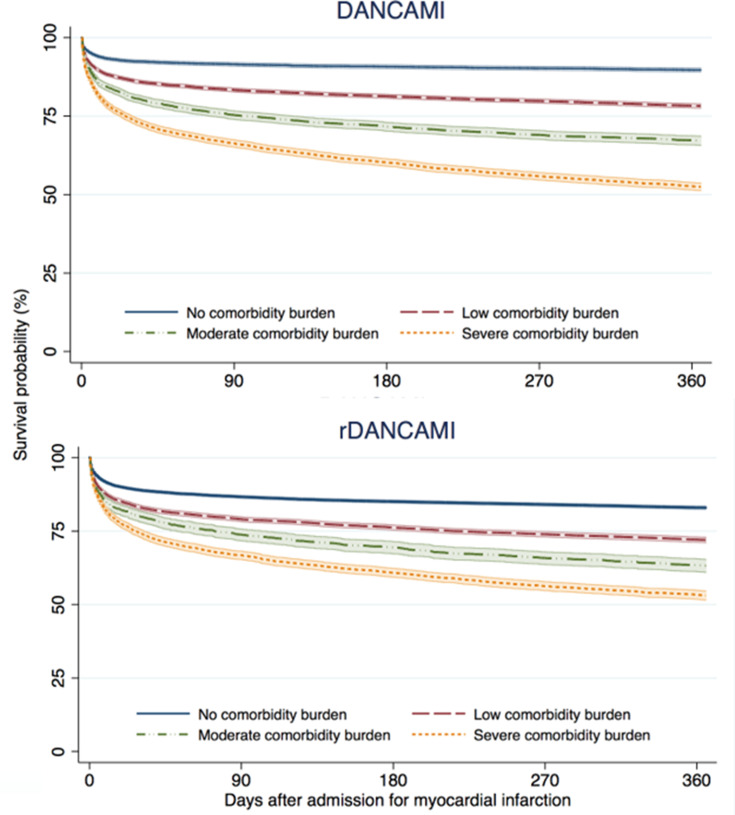
The DANCAMI included 24 comorbidities. The rDANCAMI included 17 non-cardiovascular comorbidities. In the Danish cohort, the DANCAMI indices outperformed both the Charlson and the Elixhauser comorbidity indices on all performance measures. The DANCAMI indices included multiple variables that were significant predictors of 1-year mortality even after controlling for all variables in the Charlson Comorbidity Index. These novel variables included valvular heart disease (hazard ratio for 1-year mortality=1.25, 95% CI: 1.14-1.35), coagulopathy (1.13, 95% CI: 1.05-1.22), alcohol and drug abuse (1.35, 95% CI: 1.15-1.58), schizophrenia (1.60, 95% CI: 1.46-1.76), affective disorder (1.29, 95% CI: 1.22-1.36), epilepsy (1.26, 95% CI: 1.05-1.50), neurodegenerative disorder (1.30, 95% CI: 1.10-1.54) and chronic pancreatitis (1.71, 95% CI: 1.14-2.56). The results were supported by the external validation in New Zealand.
DANCAMI assessed comorbidity burden of patients with first-time myocardial infarction, outperformed existing comorbidity indices, and was generalizable to patients outside Denmark. DANCAMI is recommended as a standard approach for comorbidity adjustment in studies of myocardial infarction prognosis.
开发并验证丹麦急性心肌梗死合并症指数(DANCAMI),用于在心肌梗死预后研究中调整合并症负担。
利用医学登记数据,我们确定了2000年至2013年丹麦首次发生心肌梗死的患者(n = 36,685)。我们开发了合并症指数,用于预测所有合并症导致的1年全因死亡率(DANCAMI),并将其限制在非心血管合并症(rDANCAMI)。对于变量选择,我们使用多变量Cox模型的风险比逐步消除合并症。我们使用标准性能指标(Nagelkerke's R、Harrell's C统计量、综合判别改善和连续净重新分类指数)将DANCAMI/rDANCAMI与Charlson和Elixhauser合并症指数进行比较。我们评估了Charlson合并症指数中未包含的新型DANCAMI变量的显著性。在2007年至2016年新西兰心肌梗死患者中进行了外部验证(n = 75,069)。
DANCAMI包括24种合并症。rDANCAMI包括17种非心血管合并症。在丹麦队列中,DANCAMI指数在所有性能指标上均优于Charlson和Elixhauser合并症指数。即使在控制了Charlson合并症指数中的所有变量后,DANCAMI指数仍包含多个对1年死亡率有显著预测作用的变量。这些新型变量包括瓣膜性心脏病(1年死亡率风险比 = 1.25,95%置信区间:1.14 - 1.35)、凝血病(1.13,95%置信区间:1.05 - 1.22)、酒精和药物滥用(1.35,95%置信区间:1.15 - 1.58)、精神分裂症(1.60,95%置信区间:1.46 - 1.76)、情感障碍(1.29,95%置信区间:1.22 - 1.36)、癫痫(1.26,95%置信区间:1.05 - 1.50)、神经退行性疾病(1.30,95%置信区间:1.10 - 1.54)和慢性胰腺炎(1.71,95%置信区间:1.14 - 2.56)。新西兰的外部验证结果支持了这些结果。
DANCAMI评估了首次心肌梗死患者的合并症负担,优于现有合并症指数,并且可推广到丹麦以外的患者。建议将DANCAMI作为心肌梗死预后研究中合并症调整的标准方法。