Faculty of Pharmaceutical Sciences, University of British Columbia, Vancouver, BC, Canada.
Medical Division, CTC Communications, Mississauga, ON, Canada.
Int J Clin Pract. 2021 Aug;75(8):e13871. doi: 10.1111/ijcp.13871. Epub 2020 Dec 18.
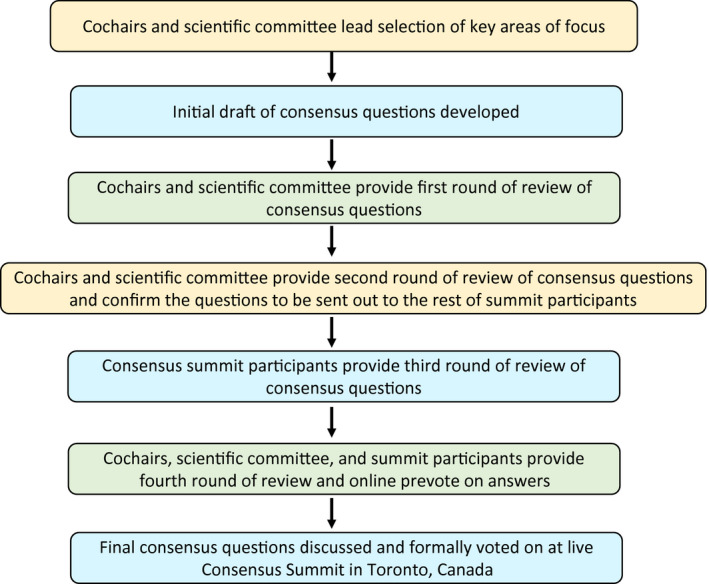
Opioid misuse and overuse have contributed to a widespread overdose crisis and many patients and physicians are considering medical cannabis to support opioid tapering and chronic pain control. Using a five-step modified Delphi process, we aimed to develop consensus-based recommendations on: 1) when and how to safely initiate and titrate cannabinoids in the presence of opioids, 2) when and how to safely taper opioids in the presence of cannabinoids and 3) how to monitor patients and evaluate outcomes when treating with opioids and cannabinoids.
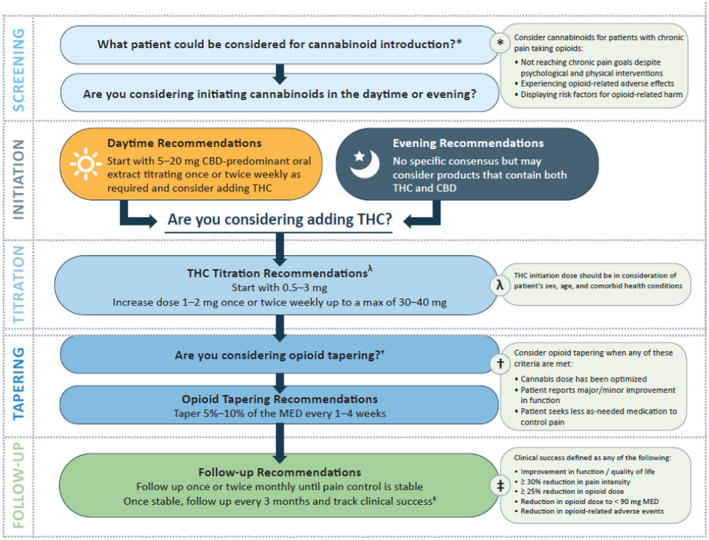
In patients with chronic pain taking opioids not reaching treatment goals, there was consensus that cannabinoids may be considered for patients experiencing or displaying opioid-related complications, despite psychological or physical interventions. There was consensus observed to initiate with a cannabidiol (CBD)-predominant oral extract in the daytime and consider adding tetrahydrocannabinol (THC). When adding THC, start with 0.5-3 mg, and increase by 1-2 mg once or twice weekly up to 30-40 mg/day. Initiate opioid tapering when the patient reports a minor/major improvement in function, seeks less as-needed medication to control pain and/or the cannabis dose has been optimised. The opioid tapering schedule may be 5%-10% of the morphine equivalent dose (MED) every 1 to 4 weeks. Clinical success could be defined by an improvement in function/quality of life, a ≥30% reduction in pain intensity, a ≥25% reduction in opioid dose, a reduction in opioid dose to <90 mg MED and/or reduction in opioid-related adverse events.
This five-stage modified Delphi process led to the development of consensus-based recommendations surrounding the safe introduction and titration of cannabinoids in concert with tapering opioids.
阿片类药物的滥用和过度使用导致了广泛的过量危机,许多患者和医生正在考虑使用医用大麻来支持阿片类药物的逐渐减少和慢性疼痛控制。我们采用五步改良德尔菲法,旨在就以下方面制定基于共识的建议:1)在存在阿片类药物的情况下,何时以及如何安全地开始和滴定大麻素;2)在存在大麻素的情况下,何时以及如何安全地减少阿片类药物;3)在使用阿片类药物和大麻素治疗时,如何监测患者和评估结果。
对于正在服用阿片类药物但未达到治疗目标的慢性疼痛患者,如果出现或显示与阿片类药物相关的并发症,尽管进行了心理或身体干预,仍有共识认为可以考虑使用大麻素。观察到的共识是,在白天开始使用 CBD 为主的口服提取物,并考虑添加四氢大麻酚(THC)。添加 THC 时,起始剂量为 0.5-3mg,每周增加 1-2mg,直至每天 30-40mg。当患者报告功能改善(轻度/重度)、寻求更少按需药物控制疼痛和/或大麻剂量已优化时,开始逐渐减少阿片类药物。阿片类药物逐渐减少的方案可以是每 1-4 周减少吗啡当量剂量(MED)的 5%-10%。临床成功可以定义为功能/生活质量的改善、疼痛强度降低≥30%、阿片类药物剂量降低≥25%、阿片类药物剂量降低至<90mg MED 以及/或减少与阿片类药物相关的不良反应。
这五个阶段的改良德尔菲法导致了在逐渐减少阿片类药物的同时安全引入和滴定大麻素的共识建议的制定。