Cazaubiel Titouan, Mulas Olga, Montes Lydia, Schavgoulidze Anaïs, Avet-Loiseau Hervé, Corre Jill, Perrot Aurore
Hematology Department, University Hospital, 33600 Bordeaux, France.
Centre de Recherche en Cancérologie de Toulouse, Institut National de la Santé et de la Recherche Médicale U1037, 31059 Toulouse, France.
Cancers (Basel). 2020 Nov 24;12(12):3497. doi: 10.3390/cancers12123497.
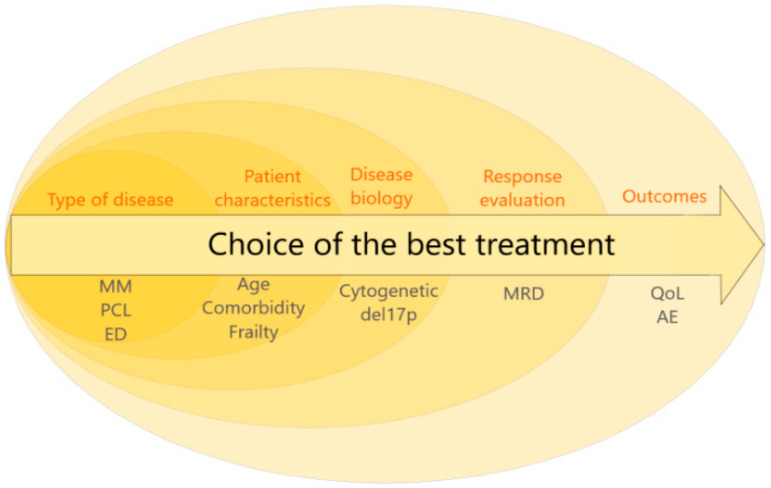
Myeloma therapeutic strategies have been adapted to patients' age and comorbidities for a long time. However, although cytogenetics and clinical presentations (plasmablastic cytology; extramedullary disease) are major prognostic factors, until recently, all patients received the same treatment whatever their initial risk. No strong evidence allows us to use a personalized treatment according to one cytogenetic abnormality in newly diagnosed myeloma. Retrospective studies showed a benefit of a double autologous transplant in high-risk cytogenetics according to the International Myeloma Working Group definition (t(4;14), t(14;16) or del(17p)). Moreover, this definition has to be updated since other independent abnormalities, namely gain 1q, del(1p32), and trisomies 5 or 21, as well as TP53 mutations, are also prognostic. Another very strong predictive tool is the response to treatment assessed by the evaluation of minimal residual disease (MRD). We are convinced that the time has come to use it to adapt the strategy to a dynamic risk. Many trials are ongoing to answer many questions: when and how should we adapt the therapy, its intensity and duration. Nevertheless, we also have to take into account the clinical outcome for one patient, especially adverse events affecting his or her quality of life and his or her preferences for continuous/fixed duration treatment.
骨髓瘤治疗策略长期以来一直根据患者的年龄和合并症进行调整。然而,尽管细胞遗传学和临床表现(浆母细胞形态学;髓外疾病)是主要的预后因素,但直到最近,所有患者无论初始风险如何都接受相同的治疗。没有强有力的证据支持我们根据新诊断骨髓瘤中的一种细胞遗传学异常来采用个性化治疗。回顾性研究表明,根据国际骨髓瘤工作组的定义(t(4;14)、t(14;16)或del(17p)),双次自体移植对高危细胞遗传学患者有益。此外,由于其他独立的异常情况,即1q增益、del(1p32)、5号或21号染色体三体以及TP53突变也具有预后意义,因此这一定义必须更新。另一个非常强大的预测工具是通过评估微小残留病(MRD)来评估治疗反应。我们坚信,现在是时候利用它来根据动态风险调整治疗策略了。许多试验正在进行,以回答许多问题:我们应该何时以及如何调整治疗、其强度和持续时间。然而,我们还必须考虑单个患者的临床结局,尤其是影响其生活质量的不良事件以及他或她对持续/固定疗程治疗的偏好。