Clinical Trials Unit, London School of Hygiene & Tropical Medicine Faculty of Epidemiology and Population Health, London, UK
Clinical Trials Unit, London School of Hygiene & Tropical Medicine Faculty of Epidemiology and Population Health, London, UK.
Emerg Med J. 2021 Apr;38(4):270-278. doi: 10.1136/emermed-2020-210424. Epub 2020 Dec 1.
Early tranexamic acid (TXA) treatment reduces head injury deaths after traumatic brain injury (TBI). We used brain scans that were acquired as part of the routine clinical practice during the CRASH-3 trial (before unblinding) to examine the mechanism of action of TXA in TBI. Specifically, we explored the potential effects of TXA on intracranial haemorrhage and infarction.
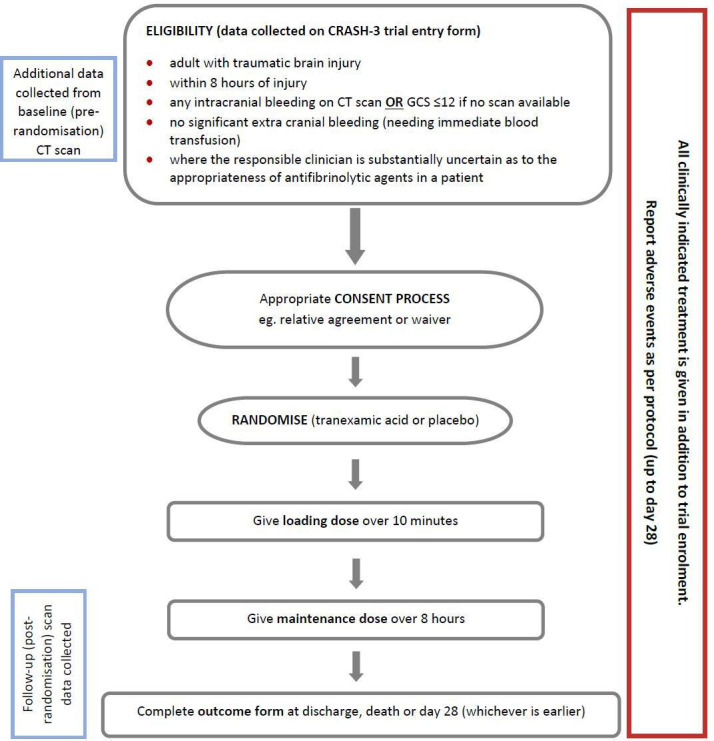
This is a prospective substudy nested within the CRASH-3 trial, a randomised placebo-controlled trial of TXA (loading dose 1 g over 10 min, then 1 g infusion over 8 hours) in patients with isolated head injury. CRASH-3 trial patients were recruited between July 2012 and January 2019. Participants in the current substudy were a subset of trial patients enrolled at 10 hospitals in the UK and 4 in Malaysia, who had at least one CT head scan performed as part of the routine clinical practice within 28 days of randomisation. The primary outcome was the volume of intraparenchymal haemorrhage (ie, contusion) measured on a CT scan done after randomisation. Secondary outcomes were progressive intracranial haemorrhage (post-randomisation CT shows >25% of volume seen on pre-randomisation CT), new intracranial haemorrhage (any haemorrhage seen on post-randomisation CT but not on pre-randomisation CT), cerebral infarction (any infarction seen on any type of brain scan done post-randomisation, excluding infarction seen pre-randomisation) and intracranial haemorrhage volume (intraparenchymal + intraventricular + subdural + epidural) in those who underwent neurosurgical haemorrhage evacuation. We planned to conduct sensitivity analyses excluding patients who were severely injured at baseline. Dichotomous outcomes were analysed using relative risks (RR) or hazard ratios (HR), and continuous outcomes using a linear mixed model.
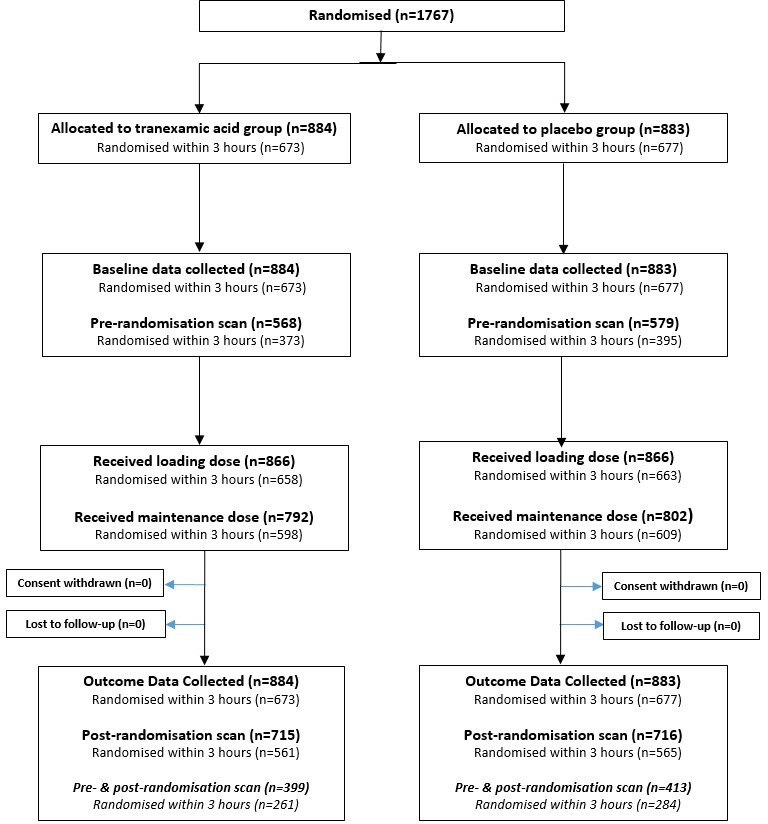
1767 patients were included in this substudy. One-third of the patients had a baseline GCS (Glasgow Coma Score) of 3 (n=579) and 24% had unilateral or bilateral unreactive pupils. 46% of patients were scanned pre-randomisation and post-randomisation (n=812/1767), 19% were scanned only pre-randomisation (n=341/1767) and 35% were scanned only post-randomisation (n=614/1767). In all patients, there was no evidence that TXA prevents intraparenchymal haemorrhage expansion (estimate=1.09, 95% CI 0.81 to 1.45) or intracranial haemorrhage expansion in patients who underwent neurosurgical haemorrhage evacuation (n=363) (estimate=0.79, 95% CI 0.57 to 1.11). In patients scanned pre-randomisation and post-randomisation (n=812), there was no evidence that TXA reduces progressive haemorrhage (adjusted RR=0.91, 95% CI 0.74 to 1.13) and new haemorrhage (adjusted RR=0.85, 95% CI 0.72 to 1.01). When patients with unreactive pupils at baseline were excluded, there was evidence that TXA prevents new haemorrhage (adjusted RR=0.80, 95% CI 0.66 to 0.98). In patients scanned post-randomisation (n=1431), there was no evidence of an increase in infarction with TXA (adjusted HR=1.28, 95% CI 0.93 to 1.76). A larger proportion of patients without (vs with) a post-randomisation scan died from head injury (38% vs 19%: RR=1.97, 95% CI 1.66 to 2.34, p<0.0001).
TXA may prevent new haemorrhage in patients with reactive pupils at baseline. This is consistent with the results of the CRASH-3 trial which found that TXA reduced head injury death in patients with at least one reactive pupil at baseline. However, the large number of patients without post-randomisation scans and the possibility that the availability of scan data depends on whether a patient received TXA, challenges the validity of inferences made using routinely collected scan data. This study highlights the limitations of using routinely collected scan data to examine the effects of TBI treatments.
ISRCTN15088122.
早期使用氨甲环酸(TXA)治疗可降低创伤性脑损伤(TBI)后的颅脑损伤死亡人数。我们使用 CRASH-3 试验(在未揭盲之前)期间作为常规临床实践的一部分获取的脑部扫描,来检查 TXA 在 TBI 中的作用机制。具体而言,我们探索了 TXA 对颅内出血和梗死的潜在影响。
这是 CRASH-3 试验的一项前瞻性嵌套子研究,该试验是一项 TXA(负荷剂量 1g 静脉输注 10 分钟,然后 1g 输注 8 小时)治疗单纯性颅脑损伤患者的随机安慰剂对照试验。CRASH-3 试验的患者于 2012 年 7 月至 2019 年 1 月期间招募。当前子研究的参与者是在英国的 10 家医院和马来西亚的 4 家医院入组的试验患者的一个子集,他们在随机分组后 28 天内至少进行了一次 CT 头部扫描作为常规临床实践的一部分。主要结局是随机分组后 CT 扫描显示的脑实质出血(即挫伤)体积。次要结局包括进行性颅内出血(随机分组后 CT 显示的体积比随机分组前 CT 显示的体积增加>25%)、新的颅内出血(随机分组后 CT 显示但随机分组前 CT 未显示的任何出血)、脑梗死(随机分组后任何类型的脑部扫描均可见的任何梗死,不包括随机分组前可见的梗死)和行神经外科血肿清除术患者的颅内出血体积(脑实质内+脑室内+硬膜下+硬膜外)。我们计划进行敏感性分析,排除基线严重损伤的患者。二分类结局采用相对风险(RR)或危险比(HR)进行分析,连续结局采用线性混合模型进行分析。
本子研究纳入了 1767 名患者。三分之一的患者基线格拉斯哥昏迷评分(GCS)为 3(n=579),24%的患者单侧或双侧瞳孔无反应。46%的患者在随机分组前和随机分组后进行了扫描(n=812),24%的患者仅在随机分组前进行了扫描(n=341),35%的患者仅在随机分组后进行了扫描(n=614)。在所有患者中,没有证据表明 TXA 可防止脑实质出血扩大(估计值=1.09,95%CI 0.81 至 1.45)或行神经外科血肿清除术患者的颅内出血扩大(n=363)(估计值=0.79,95%CI 0.57 至 1.11)。在随机分组前和随机分组后进行扫描的患者(n=812)中,没有证据表明 TXA 可减少进行性出血(调整 RR=0.91,95%CI 0.74 至 1.13)和新出血(调整 RR=0.85,95%CI 0.72 至 1.01)。当排除基线时瞳孔无反应的患者后,有证据表明 TXA 可预防新的出血(调整 RR=0.80,95%CI 0.66 至 0.98)。在随机分组后进行扫描的患者(n=1431)中,没有证据表明 TXA 会增加梗死的发生率(调整 HR=1.28,95%CI 0.93 至 1.76)。没有进行随机分组后扫描的患者中,死于颅脑损伤的比例高于进行了随机分组后扫描的患者(38% vs 19%:RR=1.97,95%CI 1.66 至 2.34,p<0.0001)。
TXA 可能预防基线时瞳孔有反应的患者发生新的出血。这与 CRASH-3 试验的结果一致,该试验发现 TXA 降低了基线时至少有一个瞳孔有反应的患者的颅脑损伤死亡人数。然而,大量患者没有进行随机分组后的扫描,并且扫描数据的可用性可能取决于患者是否接受了 TXA,这对使用常规收集的扫描数据得出的结论提出了挑战。本研究强调了使用常规收集的扫描数据来检查 TBI 治疗效果的局限性。
ISRCTN85323532。