Ravikanth Reddy
Department of Radiology, Holy Family Hospital, Thodupuzha, Kerala, India.
Indian J Radiol Imaging. 2020 Jul-Sep;30(3):344-353. doi: 10.4103/ijri.IJRI_419_19. Epub 2020 Oct 15.
Erectile dysfunction (ED) is an inability to achieve and maintain erectile rigidity sufficient for satisfactory sexual performance. It is either organic or psychogenic in origin. This study was aimed at establishing vasculogenic causes among patients being evaluated for ED using Penile Doppler Ultrasound.
Fifty-two consecutive patients with the clinical diagnosis of ED were evaluated with color Doppler ultrasound scan using a 7.5 MHz high-frequency linear transducer between July 2016 and June 2019. The examination was commenced 3 min after an intracavernosal injection with 10-20 μg of PGE and continued for 30 min. The measurements were obtained alternately from both deep penile arteries. The variables analyzed were the peak systolic velocity (PSV), end-diastolic velocity (EDV) and resistive index (RI), calculated as (PSV-EDV)/PSV. Erection Hardness was evaluated subjectively using the EH Score (EHS), a 5-point response score denoting how the patient would rate his erection. ED was subjectively assessed using the International Index of Erectile Function (IIEF-5) questionnaire. In patients with a diagnosis of vasculogenic ED, intracavernosal PGE injection was started with a 5 μg dose and then increased in 5 μg increments until the final dose of 20 μg was reached.
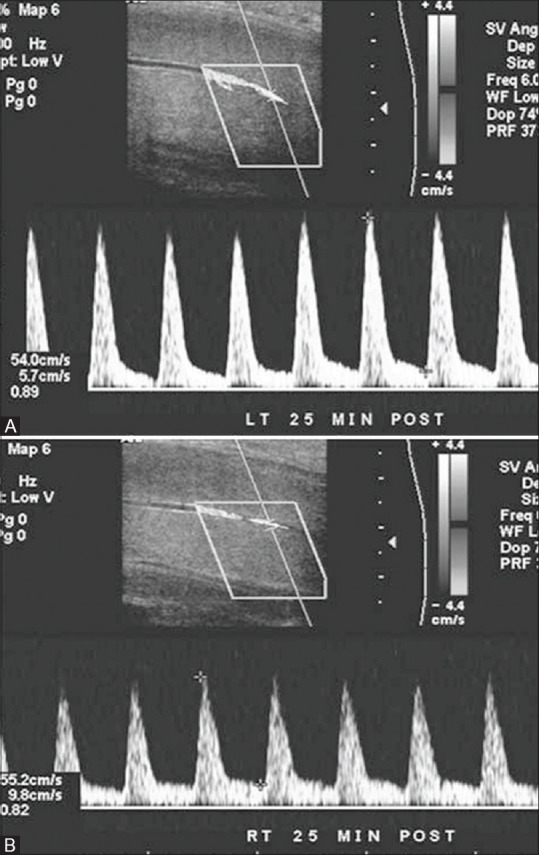
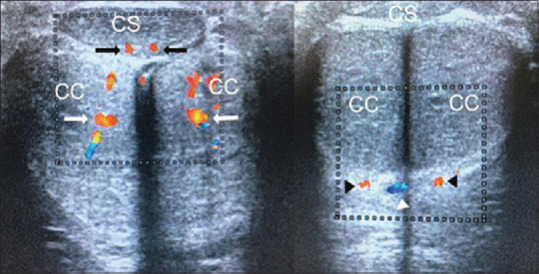
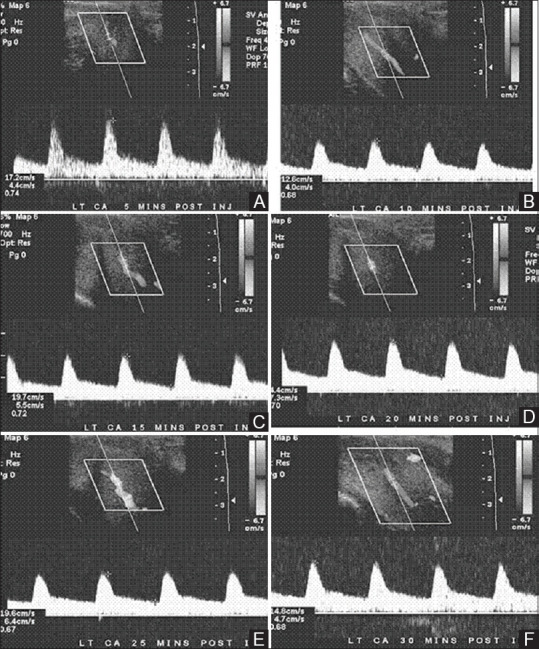
PSV of cavernosal arteries (CA) varied between 19.2 and 106.2 cm/s (mean: 43.8 ± 18.2) among the entire patients and between 19.7 and 80.2 cm/s (mean: 42.6 ± 11.3) among patients with arteriogenic ED. Arteriogenic ED was found in 8 patients (15.3%), while venogenic ED was observed in 12 patients, which constituted 23% of the entire study population and mixed arteriogenic-venogenic ED was found in 6 patients (11.5%) of the study population. DICC performed on patients diagnosed with venogenic ED on color Doppler ultrasonography revealed venous leakage and no statistically significant differences between results of DICC and color Doppler ultrasonography were found in EDV, RI, and PI measurements (P< 0.005). Among patients with venogenic ED and mixed arteriogenic-venogenic ED,2 patients had a normal erectile response and the remaining 16 received 2 mg phentolamine. A significant increase in PSV between baseline and 20 mg PGE1 ( < 0.001) was observed in all cases. Following phentolamine, there was a significant increase in grade of erection ( = 0.0001) and a significant reduction in the EDV ( = 0.0001). A reduction of the EDV to below 0.0 cm/s was observed in 12 patients. In patients with arteriogenic erectile dysfunction, mean (±standard deviation) duration of erection for consecutive doses of PGE5 μg, 10 μg, 15 μg, and 20 μg were 42.2±18.4, 55.4±24.1, 66.1 ± 31.1, and 83.3±36.7 minutes, respectively, with significant increase for each dose. In patients with veno-occlusive dysfunction, mean durations of erection significantly increased from 9.1±8.0 minutes at 10 μg to 19.2±9.8 minutes at 20 μg.
In the current study, 50% of patients had vasculogenic ED and "false-positive'' diagnosis of venous leakage was unmasked by phentolamine re-dosing. It is therefore imperative that patients with ED benefit from duplex color Doppler ultrasonography which is safe, cheap and non-ionizing diagnostic modality before initiating therapy as ED treatment is cause specific.
勃起功能障碍(ED)是指无法达到并维持足以实现满意性行为的勃起硬度。其病因要么是器质性的,要么是心因性的。本研究旨在通过阴茎多普勒超声检查,确定接受ED评估的患者中的血管源性病因。
2016年7月至2019年6月期间,对52例临床诊断为ED的连续患者,使用7.5MHz高频线性探头进行彩色多普勒超声扫描评估。在海绵体内注射10 - 20μg前列腺素E(PGE)3分钟后开始检查,并持续30分钟。从双侧阴茎深动脉交替进行测量。分析的变量包括收缩期峰值流速(PSV)、舒张末期流速(EDV)和阻力指数(RI),计算方法为(PSV - EDV)/PSV。使用勃起硬度评分(EHS)主观评估勃起硬度,EHS是一个5分制的反应评分,表示患者对其勃起的评价。使用国际勃起功能指数(IIEF - 5)问卷主观评估ED。对于诊断为血管源性ED的患者,海绵体内PGE注射起始剂量为5μg,然后以5μg的增量增加,直至达到最终剂量20μg。
在所有患者中,海绵体动脉(CA)的PSV在19.2至106.2cm/s之间(平均:43.8±18.2),在动脉源性ED患者中在19.7至80.2cm/s之间(平均:42.6±11.3)。发现8例患者(15.3%)患有动脉源性ED,12例患者观察到静脉源性ED,占整个研究人群的23%,6例患者(11.5%)发现混合性动脉 - 静脉源性ED。对彩色多普勒超声诊断为静脉源性ED的患者进行海绵体药物注射血管造影(DICC),显示静脉漏,并且在EDV、RI和PI测量中,DICC结果与彩色多普勒超声检查结果之间未发现统计学显著差异(P<0.005)。在静脉源性ED和混合性动脉 - 静脉源性ED患者中,2例患者勃起反应正常,其余16例接受了2mg酚妥拉明治疗。在所有病例中,观察到从基线到20mg PGE1时PSV显著增加(<0.001)。使用酚妥拉明后,勃起等级显著增加(=0.0001),EDV显著降低(=0.0001)。12例患者的EDV降低至0.0cm/s以下。在动脉源性勃起功能障碍患者中,连续剂量的PGE 5μg、10μg、15μg和20μg时的平均(±标准差)勃起持续时间分别为42.2±18.4、55.4±24.1、