Department of Internal Medicine and Cardiology, Charité-Universitätsmedizin Berlin, Campus Virchow-Klinikum, Augustenburger Platz 1, Berlin, 13353, Germany.
DZHK (German Centre for Cardiovascular Research), Partner Site, Berlin, Germany.
ESC Heart Fail. 2021 Feb;8(1):333-343. doi: 10.1002/ehf2.13075. Epub 2020 Dec 6.
This study aimed to evaluate the impact of coronavirus disease 2019 (Covid-19) outbreak on admissions for acute myocardial infarction (AMI) and related mortality, severity of presentation, major cardiac complications and outcome in a tertiary-care university hospital in Berlin, Germany.
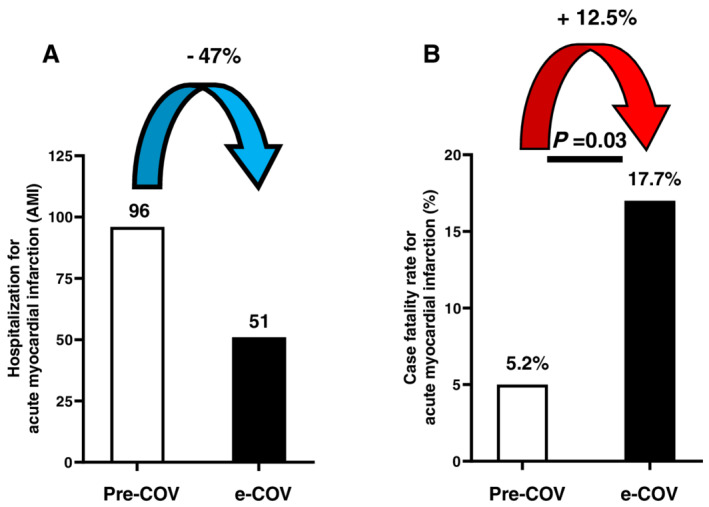
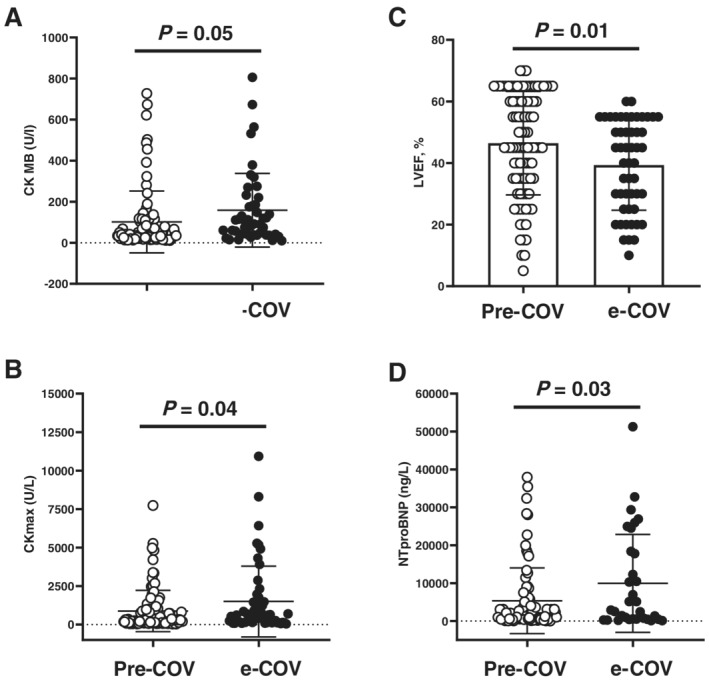
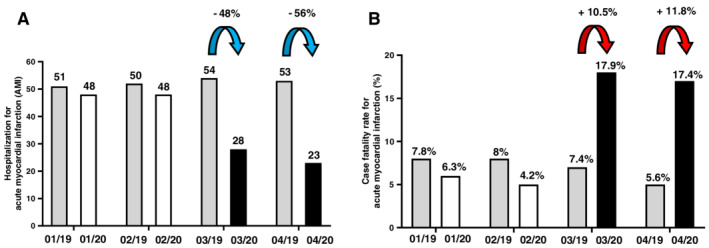
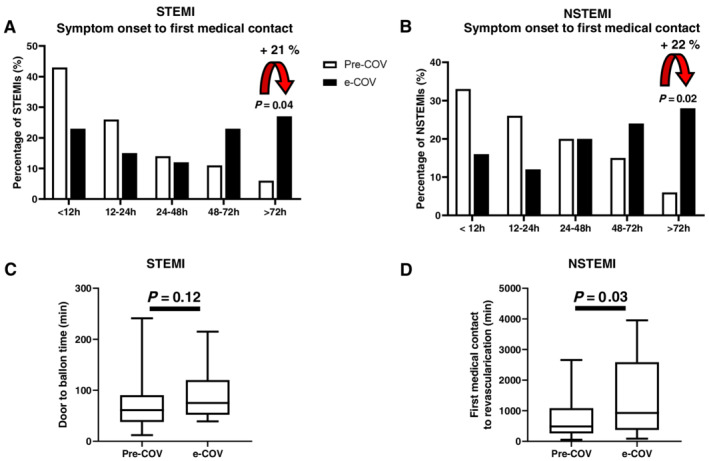
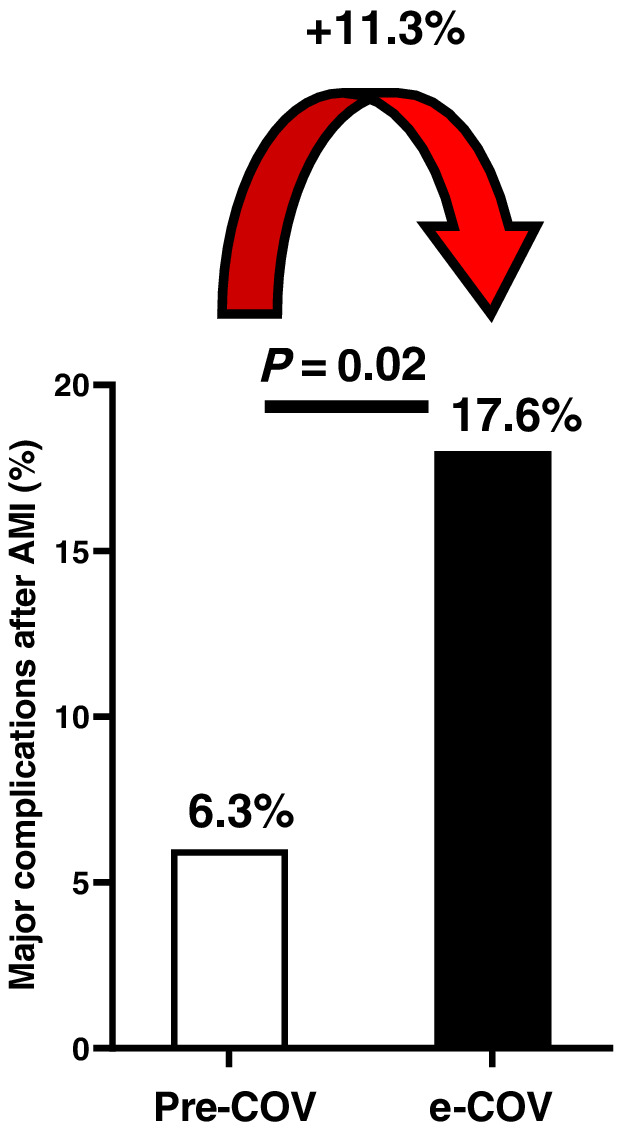
In a single-centre cross-sectional observational study, we included 355 patients with AMI containing ST-elevation or non-ST-elevation myocardial infarction (STEMI or NSTEMI), admitted for emergency cardiac catheterization between January and April 2020 and the equivalent time in 2019. During the early phase of the Covid-19 pandemic (e-COV) in Berlin (March and April 2020), admissions for AMI halved compared with those in the pre-Covid-19 time (January and February 2020; pre-COV) and with those in the corresponding months in 2019. However, mortality for AMI increased substantially from 5.2% pre-COV to 17.7% (P < 0.05) during e-COV. Severity of presentation for AMI was more pronounced during e-COV [increased levels of cardiac enzymes, reduced left ventricular ejection fraction (LVEF), an increase in the need of inotropic support by 25% (P < 0.01)], while patients' demographic and angiographic characteristics did not differ between pre-COV and e-COV. Time from symptom onset to first medical contact was prolonged in all AMI during e-COV (presentation > 72 h +21% in STEMI, p = 0.04 and presentation > 72 h in NSTEMI +22%, p = 0.02). Door to balloon time was similar in STEMI patients, while time from first medical contact to revascularization was significantly delayed in NSTEMI patients (p = 0.02). Major cardiac complications after AMI occurred significantly more often, and cardiac recovery was worse in e-COV than in pre-COV, demonstrated by a significantly lower LVEF (39 ± 16 vs. 46 ± 16, p < 0.05) at hospital discharge and substantially higher NTproBNP levels.
The Covid-19 outbreak affects hospital admissions for acute coronary syndromes. During the first phase of the pandemia, significantly less patients with AMI were admitted, but those admitted presented with a more severe phenotype and had a higher mortality, more complications, and a worse short-term outcome. Therefore, our data indicate that Covid-19 had relevant impact on non-infectious disease states, such as acute coronary syndromes.
本研究旨在评估 2019 年冠状病毒病(COVID-19)大流行对德国柏林一家三级保健大学医院急性心肌梗死(AMI)入院人数和相关死亡率、发病严重程度、主要心脏并发症及预后的影响。
在一项单中心横断面观察性研究中,我们纳入了 2020 年 1 月至 4 月和 2019 年同期因急性心肌梗死行紧急冠状动脉造影的 355 例 ST 段抬高或非 ST 段抬高心肌梗死(STEMI 或 NSTEMI)患者。在柏林 COVID-19 大流行早期(2020 年 3 月和 4 月),AMI 入院人数与 COVID-19 前时期(2020 年 1 月和 2 月)相比减半,与 2019 年同期相比减半。然而,AMI 的死亡率在 COVID-19 大流行早期显著增加,从 COVID-19 前时期的 5.2%增加到 17.7%(P<0.05)。在 COVID-19 大流行早期,AMI 的发病严重程度更为明显[心肌酶水平升高、左心室射血分数(LVEF)降低、正性肌力支持需求增加 25%(P<0.01)],而 COVID-19 前时期和 COVID-19 大流行早期患者的人口统计学和血管造影特征无差异。在所有 AMI 患者中,COVID-19 大流行早期症状发作至首次医疗接触的时间延长(STEMI 中表现超过 72 小时增加 21%,p=0.04,NSTEMI 中表现超过 72 小时增加 22%,p=0.02)。STEMI 患者的门球时间相似,而 NSTEMI 患者从首次医疗接触到血运重建的时间明显延迟(p=0.02)。COVID-19 大流行早期 AMI 后主要心脏并发症发生明显更为频繁,心脏恢复情况更差,出院时 LVEF 明显降低(39±16 比 46±16,p<0.05),NT-proBNP 水平明显升高。
COVID-19 大流行影响急性冠状动脉综合征的住院人数。在大流行的第一阶段,AMI 入院人数明显减少,但入院患者的表型更为严重,死亡率更高,并发症更多,短期预后更差。因此,我们的数据表明 COVID-19 对非传染性疾病状态(如急性冠状动脉综合征)有重要影响。