Department of Clinical and Experimental Sciences, Unit of Endocrinology and Metabolism, University of Brescia, Viale Europa 11, 25123, Brescia, Italy.
Department of Clinical and Experimental Sciences, Unit of Infectious and Tropical Diseases, University of Brescia and ASST Spedali di Brescia, Brescia, Italy.
Infection. 2021 Apr;49(2):295-303. doi: 10.1007/s15010-020-01558-6. Epub 2020 Dec 8.
The prevalence of low testosterone and symptoms of hypogonadism in HIV-infected men is still debated. We aimed to estimate the prevalence and type of hypogonadism in HIV-infected males complaining about sexual symptoms, and to evaluate the role of calculated free testosterone (cFT) vs total testosterone (TT) for diagnosis. Furthermore, we evaluated relationship between sex hormone-binding globulin (SHBG), gonadal status and clinical and virologic parameters.
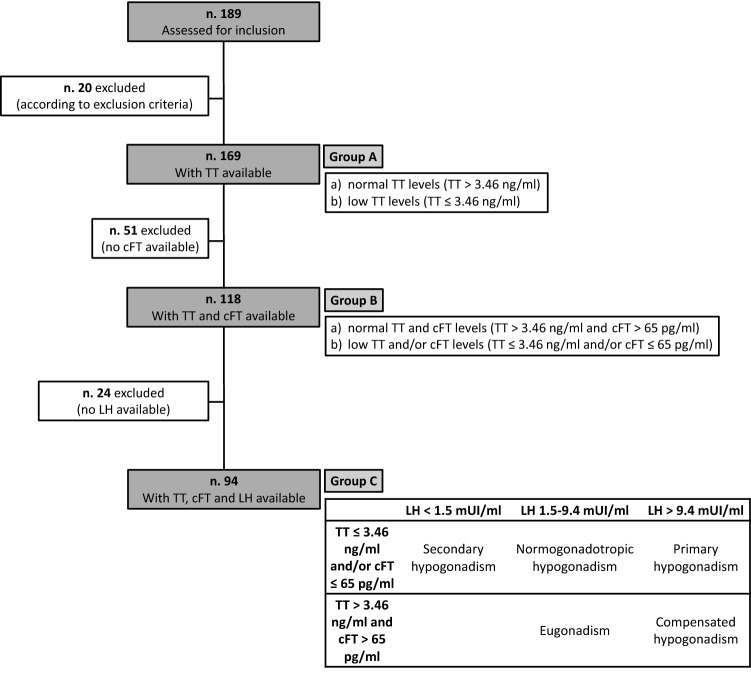
We retrospectively evaluated 169 HIV-infected men with sexual symptoms, with TT available. Among them, we selected 94 patients with TT, SHBG, cFT, and luteinizing hormone (LH) available, and classified hypogonadism into overt (low TT and/or low cFT) and compensated (high LH, normal TT and cFT). Comparison was performed by non-parametric Kruskal-Wallis test and Spearman's correlation was calculated to verify the possible associations.
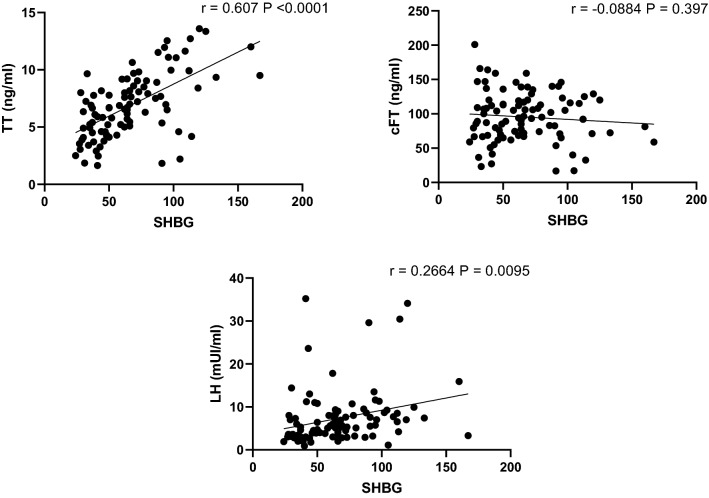
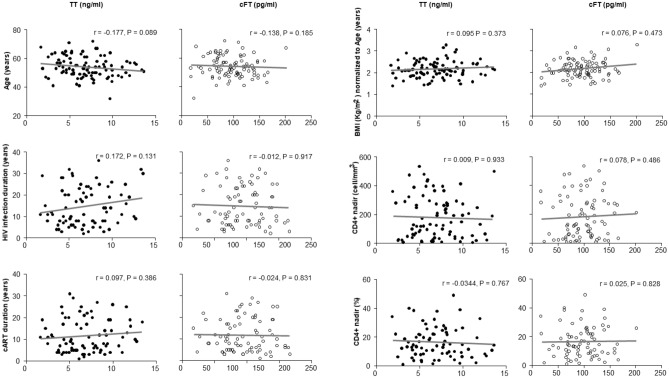
Overt and compensated hypogonadism were found in 20.2% and 13.8% of patients, respectively. With reliance on TT alone, only 10.6% of patients would have met diagnosis. SHBG values were elevated in one third of patients, and higher in men with compensated hypogonadism. Significant positive correlation was found between SHBG and HIV infection duration, TT and LH.
Only a complete hormonal profile can properly diagnose and classify hypogonadism in HIV-infected men complaining about sexual symptoms. TT alone reliance may lead to half of diagnoses missing, while lack of gonadotropin prevents the identification of compensated hypogonadism. This largely comes from high SHBG, which seems to play a central role in the pathogenesis of hypogonadism in this population.
HIV 感染男性的低睾酮和性腺功能减退症状的流行仍存在争议。我们旨在评估有性功能障碍症状的 HIV 感染男性的性腺功能减退症的患病率和类型,并评估计算游离睾酮(cFT)与总睾酮(TT)对诊断的作用。此外,我们评估了性激素结合球蛋白(SHBG)、性腺状态与临床和病毒学参数之间的关系。
我们回顾性评估了 169 例有性功能障碍症状且 TT 可检测的 HIV 感染男性。其中,我们选择了 94 例 TT、SHBG、cFT 和黄体生成素(LH)均可检测的患者,并将性腺功能减退症分为明显(TT 和/或 cFT 低)和代偿(高 LH、TT 和 cFT 正常)。采用非参数 Kruskal-Wallis 检验进行比较,并用 Spearman 相关分析来验证可能的相关性。
明显和代偿性腺功能减退症分别见于 20.2%和 13.8%的患者。仅依赖 TT,只有 10.6%的患者符合诊断。三分之一的患者 SHBG 值升高,而代偿性腺功能减退症患者的 SHBG 值更高。SHBG 与 HIV 感染持续时间、TT 和 LH 呈显著正相关。
只有完整的激素谱才能正确诊断和分类有性功能障碍症状的 HIV 感染男性的性腺功能减退症。仅依赖 TT 可能导致一半的诊断缺失,而缺乏促性腺激素则无法识别代偿性腺功能减退症。这主要归因于高 SHBG,它似乎在该人群的性腺功能减退症发病机制中发挥核心作用。