Medicine, The University of British Columbia Faculty of Medicine, Vancouver, British Columbia, Canada
Surgery, University of Toronto, Toronto, Ontario, Canada.
BMJ Open. 2020 Dec 7;10(12):e040768. doi: 10.1136/bmjopen-2020-040768.
The COVID-19 epidemic grows and there are clinical trials of antivirals. There is an opportunity to complement these trials with investigation of angiotensin II type 1 receptor blockers (ARBs) because an ARB (losartan) was effective in murine influenza pneumonia.
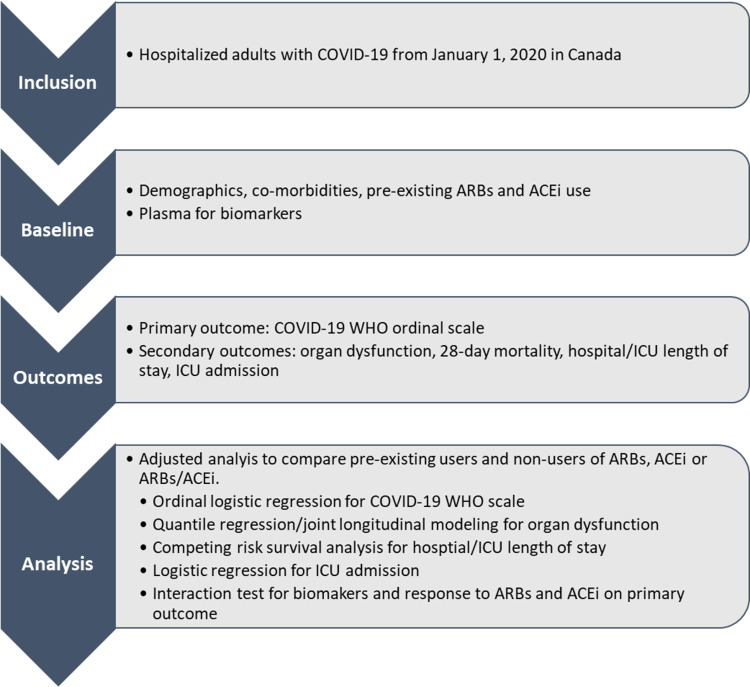
Our innovative design includes: ARBs; alignment with the WHO Ordinal Scale (primary endpoint) to align with other COVID-19 trials; joint longitudinal analysis; and predictive biomarkers (angiotensins I, 1-7, II and ACE1 and ACE2). Our hypothesis is: ARBs decrease the need for hospitalisation, severity (need for ventilation, vasopressors, extracorporeal membrane oxygenation or renal replacement therapy) or mortality of hospitalised COVID-19 infected adults. Our two-pronged multicentre pragmatic observational cohort study examines safety and effectiveness of ARBs in (1) hospitalised adult patients with COVID-19 and (2) out-patients already on or not on ARBs. The primary outcome will be evaluated by ordinal logistic regression and main secondary outcomes by both joint longitudinal modelling analyses. We will compare rates of hospitalisation of ARB-exposed versus not ARB-exposed patients. We will also determine whether continuing ARBs or not decreases the primary outcome. Based on published COVID-19 cohorts, assuming 15% of patients are ARB-exposed, a total sample size of 497 patients can detect a proportional OR of 0.5 (alpha=0.05, 80% power) comparing WHO scale of ARB-exposed versus non-ARB-exposed patients.
This study has core institution approval (UBC Providence Healthcare Research Ethics Board) and site institution approvals (Health Research Ethics Board, University of Alberta; Comite d'etique de la recerche, CHU Sainte Justine (for McGill University and University of Sherbrook); Conjoint Health Research Ethics Board, University of Calgary; Queen's University Health Sciences & Affiliated Hospitals Research Ethics Board; Research Ethics Board, Sunnybrook Health Sciences Centre; Veritas Independent Research Board (for Humber River Hospital); Mount Sinai Hospital Research Ethics Board; Unity Health Toronto Research Ethics Board, St. Michael's Hospital). Results will be disseminated by peer-review publication and social media releases.
NCT04510623.
COVID-19 疫情不断蔓延,目前正在进行抗病毒药物的临床试验。有机会通过研究血管紧张素 II 型 1 型受体阻滞剂 (ARB) 来补充这些试验,因为 ARB(氯沙坦)在鼠流感肺炎中是有效的。
我们的创新设计包括:ARB;与世界卫生组织(WHO)等级量表(主要终点)对齐,与其他 COVID-19 试验对齐;联合纵向分析;以及预测生物标志物(血管紧张素 I、1-7、II 和 ACE1 和 ACE2)。我们的假设是:ARB 可降低住院、严重程度(需要通气、血管加压药、体外膜氧合或肾脏替代治疗)或住院 COVID-19 感染成年人的死亡率的需求。我们的两部分多中心实用观察队列研究检查了 ARB 在(1)住院 COVID-19 成年患者中的安全性和有效性,以及(2)已经接受或未接受 ARB 的门诊患者中的安全性和有效性。主要结局将通过有序逻辑回归评估,主要次要结局将通过联合纵向建模分析评估。我们将比较暴露于 ARB 和未暴露于 ARB 的患者的住院率。我们还将确定继续使用 ARB 是否会降低主要结局。根据已发表的 COVID-19 队列,假设 15%的患者暴露于 ARB,总共 497 名患者的样本量可以检测到暴露于 ARB 的患者与未暴露于 ARB 的患者的 WHO 量表的比例比值为 0.5(alpha=0.05,80%的功效)。
这项研究已获得核心机构批准(UBC Providence Healthcare 研究伦理委员会)和机构地点批准(阿尔伯塔大学健康研究伦理委员会;魁北克大学健康科学与附属医院研究伦理委员会;卡尔加里大学联合健康研究伦理委员会;皇后大学健康科学与附属医院研究伦理委员会;森尼布鲁克健康科学中心研究伦理委员会;维塔斯独立研究委员会(用于亨伯河医院);山 Sinai 医院研究伦理委员会;多伦多 Unity 健康研究伦理委员会,圣迈克尔医院)。结果将通过同行评审出版物和社交媒体发布进行传播。
NCT04510623。