Department of Endocrinology, Nanjing First Hospital, Nanjing Medical University, Nanjing 210012, China.
J Diabetes Res. 2020 Nov 24;2020:6666403. doi: 10.1155/2020/6666403. eCollection 2020.
To evaluate the effect of an inhibitor of sodium-glucose cotransporter 2 (SGLT-2 inhibitor, dapagliflozin) on glycemic variability in type 2 diabetes mellitus (T2D) under insulin glargine combined with oral hypoglycemic drugs, using a continuous glucose monitoring system (CGMS).
This prospective, self-controlled, single-center clinical trial recruited 36 patients with T2D under combined insulin glargine and oral hypoglycemic drugs. General clinical data were collected. Fasting blood glucose (FBG), postprandial blood glucose (PBG), glycosylated hemoglobin (HbA1c), and C-peptide levels were assessed before and four weeks of dapagliflozin (10 mg per day) treatment. Blood glucose was monitored for 72 hours before and after treatment using CGMS.
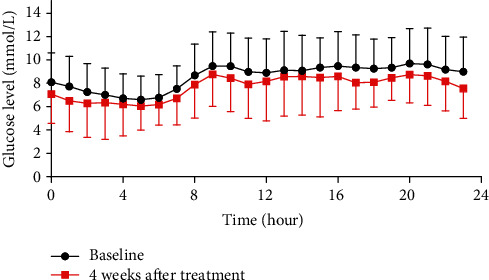
After treatment with dapagliflozin, FBG decreased from 6.74 ± 1.78 to 5.95 ± 1.13 mmol/L ( < 0.05); PBG decreased from 13.04 ± 2.99 to 10.92 ± 3.26 mmol/L ( < 0.05); HbA1c decreased from 7.37 ± 0.96% to 6.94 ± 0.80%. The proportion of patients with HbA1c < 7% increased from 27.8% to 58.3%, and the proportion of patients with HbA1c < 7% and without level 2 hypoglycemia increased from 27.8% to 55.6% ( < 0.05). CGMS data showed reduction of the 24 h MBG, MAGE, time-above-range (TAR, >10 mmol/L), high blood glucose index (HBGI), glucose management indicator (GMI), and incremental area under the curve of the glucose level more than 10 mmol/L (AUC > 10) and an increase of time-in-range (TIR, 3.9-10 mmol/L) with treatment. Homeostasis model assessment for pancreatic beta-cell function (HOMA-beta) increased significantly with treatment ( < 0.05), and fewer insulin doses were required after the treatment, without increasing in hypoglycemia and urinary tract infection. Further, a stratified analysis showed that patients with higher pretreatment HbA1c and waist-to-hip ratio (WHR) had greater improvement in glycemic control.
Dapagliflozin may reduce blood glucose levels, ameliorate glycemic variability, and improve pancreatic beta-cell function in patients with T2D under insulin glargine combined with other oral hypoglycemic drugs, especially in those with poor glucose control and abdominal obesity.
使用连续血糖监测系统(CGMS)评估钠-葡萄糖共转运蛋白 2 抑制剂(SGLT-2 抑制剂,达格列净)对接受甘精胰岛素联合口服降糖药治疗的 2 型糖尿病(T2D)患者血糖变异性的影响。
这项前瞻性、自身对照、单中心临床试验纳入了 36 例正在接受甘精胰岛素联合口服降糖药治疗的 T2D 患者。收集了一般临床数据。在开始达格列净(每天 10mg)治疗前和治疗后 4 周评估空腹血糖(FBG)、餐后血糖(PBG)、糖化血红蛋白(HbA1c)和 C 肽水平。在治疗前后使用 CGMS 监测 72 小时血糖。
达格列净治疗后,FBG 从 6.74 ± 1.78mmol/L 降至 5.95 ± 1.13mmol/L(<0.05);PBG 从 13.04 ± 2.99mmol/L 降至 10.92 ± 3.26mmol/L(<0.05);HbA1c 从 7.37 ± 0.96%降至 6.94 ± 0.80%。HbA1c<7%的患者比例从 27.8%增加到 58.3%,HbA1c<7%且无 2 级低血糖的患者比例从 27.8%增加到 55.6%(<0.05)。CGMS 数据显示,24 小时 MBG、MAGE、血糖高于目标范围时间(TAR,>10mmol/L)、高血糖指数(HBGI)、血糖管理指标(GMI)和血糖水平高于 10mmol/L 的增量曲线下面积(AUC>10)减少,血糖在目标范围内时间(TIR,3.9-10mmol/L)增加。治疗后,胰岛β细胞功能的稳态模型评估(HOMA-β)显著增加(<0.05),且胰岛素用量减少,低血糖和尿路感染无增加。此外,分层分析显示,治疗前 HbA1c 和腰臀比(WHR)较高的患者血糖控制改善更明显。
达格列净可降低接受甘精胰岛素联合其他口服降糖药治疗的 T2D 患者的血糖水平,改善血糖变异性,改善胰岛β细胞功能,尤其是对血糖控制较差和腹型肥胖的患者。