Lynch Charlotte, Reguilon Irene, Langer Deanna L, Lane Damon, De Prithwish, Wong Wai-Lup, Mckiddie Fergus, Ross Andrew, Shack Lorraine, Win Thida, Marshall Christopher, Revheim Mona-Eliszabeth, Danckert Bolette, Butler John, Dizdarevic Sabina, Louzado Cheryl, Mcgivern Canice, Hazlett Anne, Chew Cindy, O'connell Martin, Harrison Samantha
International Cancer Benchmarking Partnership (ICBP), Policy & Information, Cancer Research UK, 2 2 Redman Place, London, E20 1JQ, UK.
Brand & Strategy, eConsult Health Ltd, 46-48 East Street, Surrey, KT17 1HQ, UK.
Int J Qual Health Care. 2021 Feb 20;33(1). doi: 10.1093/intqhc/mzaa166.
To explore differences in position emission tomography-computed tomography (PET-CT) service provision internationally to further understand the impact variation may have upon cancer services. To identify areas of further exploration for researchers and policymakers to optimize PET-CT services and improve the quality of cancer services.
Comparative analysis using data based on pre-defined PET-CT service metrics from PET-CT stakeholders across seven countries. This was further informed via document analysis of clinical indication guidance and expert consensus through round-table discussions of relevant PET-CT stakeholders. Descriptive comparative analyses were produced on use, capacity and indication guidance for PET-CT services between jurisdictions.
PET-CT services across 21 jurisdictions in seven countries (Australia, Denmark, Canada, Ireland, New Zealand, Norway and the UK).
None.
INTERVENTION(S): None.
MAIN OUTCOME MEASURE(S): None.
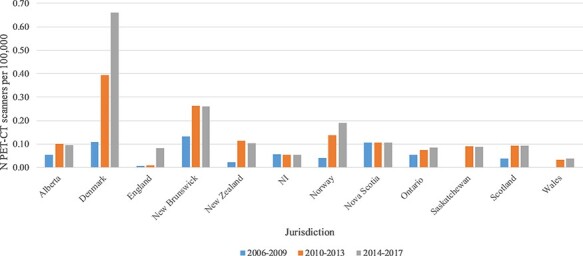
PET-CT service provision has grown over the period 2006-2017, but scale of increase in capacity and demand is variable. Clinical indication guidance varied across countries, particularly for small-cell lung cancer staging and the specific acknowledgement of gastric cancer within oesophagogastric cancers. There is limited and inconsistent data capture, coding, accessibility and availability of PET-CT activity across countries studied.
Variation in PET-CT scanner quantity, acquisition over time and guidance upon use exists internationally. There is a lack of routinely captured and accessible PET-CT data across the International Cancer Benchmarking Partnership countries due to inconsistent data definitions, data linkage issues, uncertain coverage of data and lack of specific coding. This is a barrier in improving the quality of PET-CT services globally. There needs to be greater, richer data capture of diagnostic and staging tools to facilitate learning of best practice and optimize cancer services.
探讨国际上正电子发射断层扫描-计算机断层扫描(PET-CT)服务提供情况的差异,以进一步了解这种差异可能对癌症服务产生的影响。确定研究人员和政策制定者进一步探索的领域,以优化PET-CT服务并提高癌症服务质量。
使用来自七个国家PET-CT利益相关者基于预定义PET-CT服务指标的数据进行比较分析。通过对临床适应症指南的文献分析以及相关PET-CT利益相关者圆桌讨论达成的专家共识,进一步完善了该分析。对各辖区之间PET-CT服务的使用、能力和适应症指南进行了描述性比较分析。
七个国家(澳大利亚、丹麦、加拿大、爱尔兰、新西兰、挪威和英国)21个辖区的PET-CT服务。
无。
无。
无。
2006年至2017年期间,PET-CT服务有所增长,但能力和需求的增长规模各不相同。各国的临床适应症指南存在差异,特别是在小细胞肺癌分期以及食管癌和胃癌中对胃癌的具体认定方面。在所研究的国家中,PET-CT活动的数据收集、编码、可及性和可用性有限且不一致。
国际上PET-CT扫描仪数量、随时间的购置情况以及使用指南存在差异。由于数据定义不一致、数据链接问题、数据覆盖范围不确定以及缺乏特定编码,国际癌症基准伙伴关系国家缺乏常规收集且可获取的PET-CT数据。这是提高全球PET-CT服务质量的一个障碍。需要对诊断和分期工具进行更丰富的数据收集,以促进最佳实践的学习并优化癌症服务。