Chen Ching-Jen, Ding Dale, Lee Cheng-Chia, Kearns Kathryn N, Pomeraniec I Jonathan, Cifarelli Christopher P, Arsanious David E, Liscak Roman, Hanuska Jaromir, Williams Brian J, Yusuf Mehran B, Woo Shiao Y, Ironside Natasha, Burke Rebecca M, Warnick Ronald E, Trifiletti Daniel M, Mathieu David, Mureb Monica, Benjamin Carolina, Kondziolka Douglas, Feliciano Caleb E, Rodriguez-Mercado Rafael, Cockroft Kevin M, Simon Scott, Mackley Heath B, Zammar Samer G, Patel Neel T, Padmanaban Varun, Beatson Nathan, Saylany Anissa, Lee John Y K, Sheehan Jason P
1Department of Neurological Surgery, University of Virginia, Charlottesville, Virginia.
Departments of2Neurosurgery and.
J Neurosurg. 2020 Dec 11;135(3):742-750. doi: 10.3171/2020.7.JNS201731. Print 2021 Sep 1.
Investigations of the combined effects of neoadjuvant Onyx embolization and stereotactic radiosurgery (SRS) on brain arteriovenous malformations (AVMs) have not accounted for initial angioarchitectural features prior to neuroendovascular intervention. The aim of this retrospective, multicenter matched cohort study is to compare the outcomes of SRS with versus without upfront Onyx embolization for AVMs using de novo characteristics of the preembolized nidus.
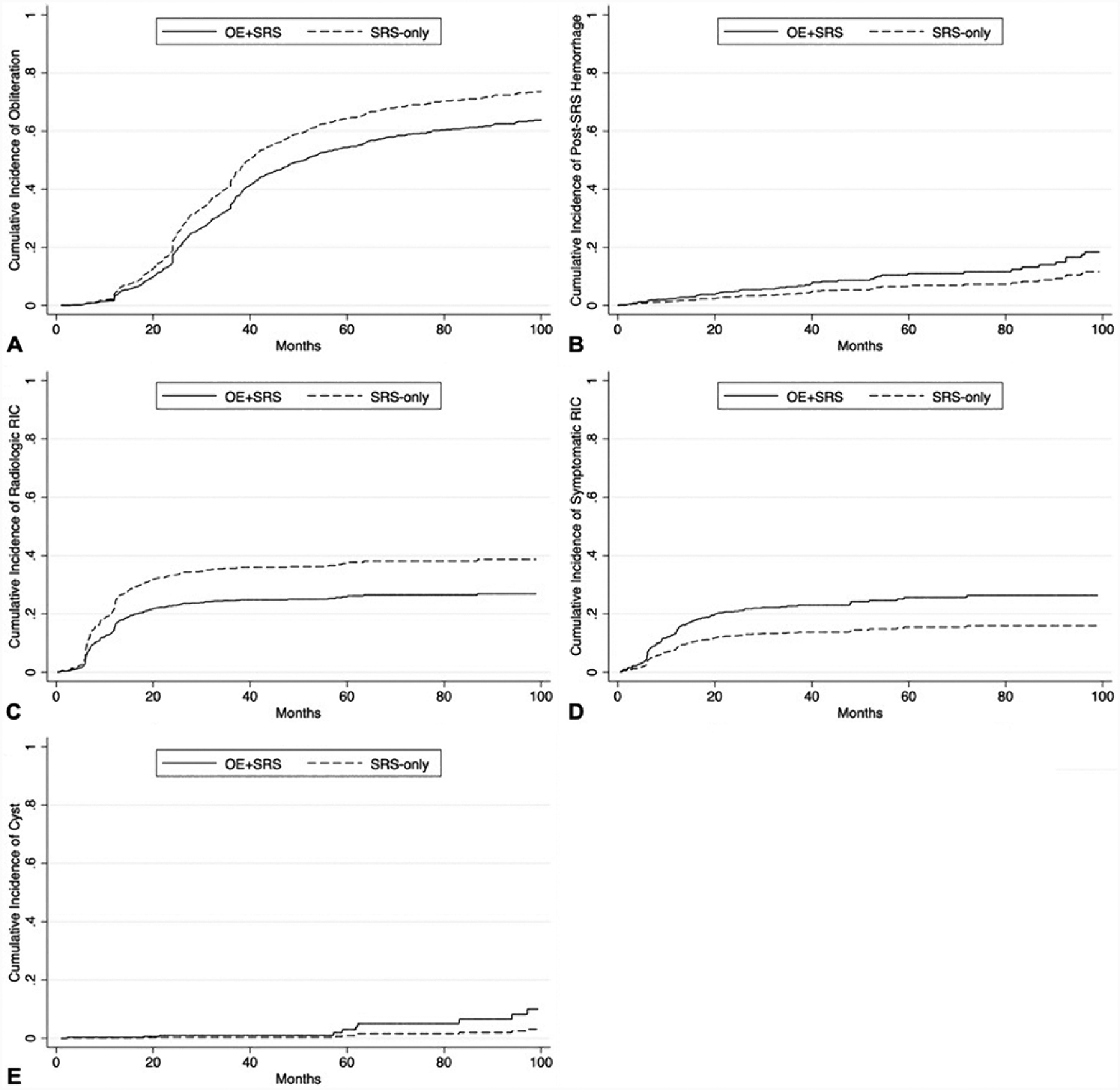
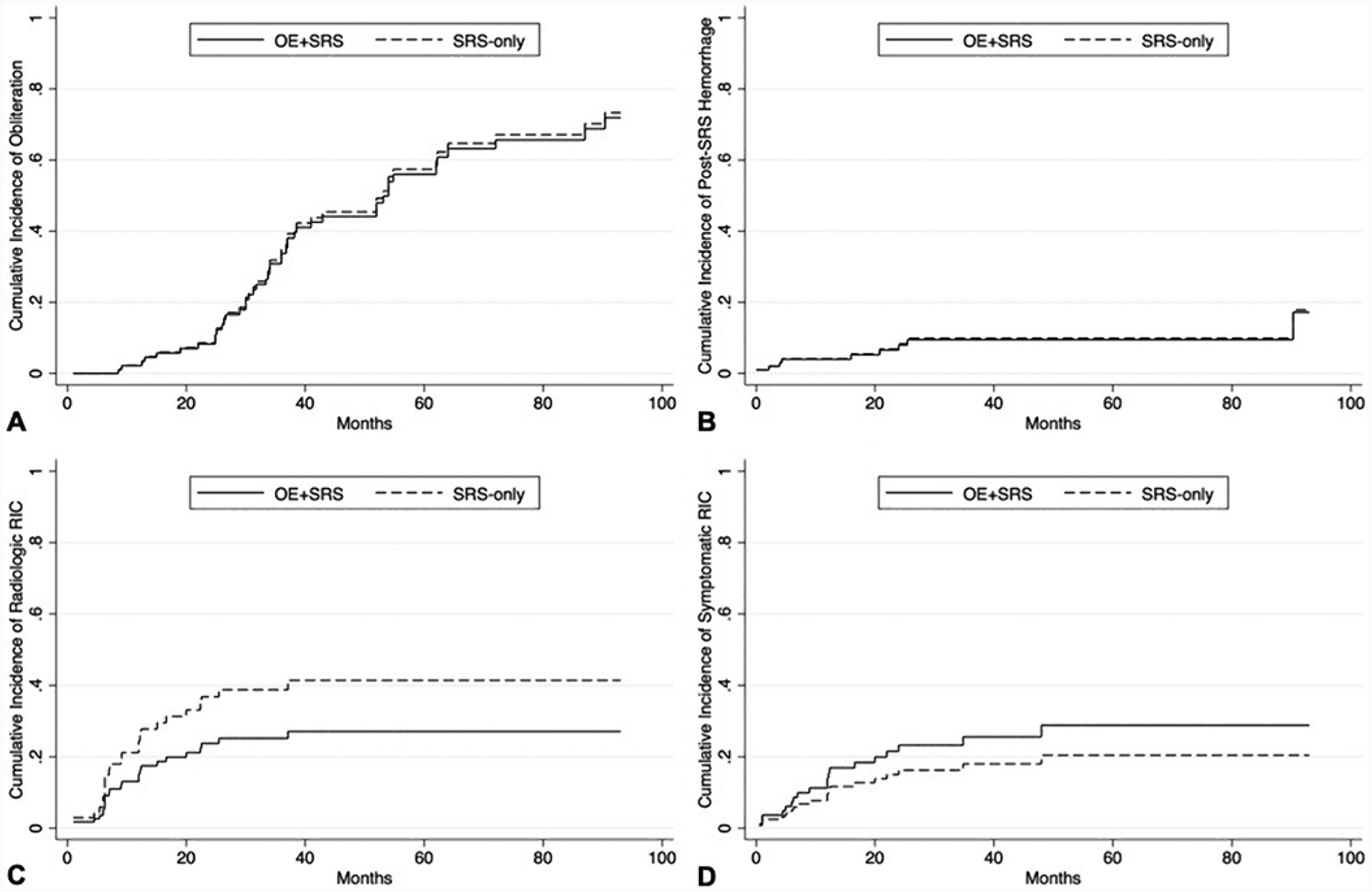
The International Radiosurgery Research Foundation AVM databases from 1987 to 2018 were retrospectively reviewed. Patients were categorized based on AVM treatment approach into Onyx embolization (OE) and SRS (OE+SRS) or SRS alone (SRS-only) cohorts and then propensity score matched in a 1:1 ratio. The primary outcome was AVM obliteration. Secondary outcomes were post-SRS hemorrhage, all-cause mortality, radiological and symptomatic radiation-induced changes (RICs), and cyst formation. Comparisons were analyzed using crude rates and cumulative probabilities adjusted for competing risk of death.
The matched OE+SRS and SRS-only cohorts each comprised 53 patients. Crude rates (37.7% vs 47.2% for the OE+SRS vs SRS-only cohorts, respectively; OR 0.679, p = 0.327) and cumulative probabilities at 3, 4, 5, and 6 years (33.7%, 44.1%, 57.5%, and 65.7% for the OE+SRS cohort vs 34.8%, 45.5%, 59.0%, and 67.1% for the SRS-only cohort, respectively; subhazard ratio 0.961, p = 0.896) of AVM obliteration were similar between the matched cohorts. The secondary outcomes of the matched cohorts were also similar. Asymptomatic and symptomatic embolization-related complication rates in the matched OE+SRS cohort were 18.9% and 9.4%, respectively.
Pre-SRS AVM embolization with Onyx does not appear to negatively influence outcomes after SRS. These analyses, based on de novo nidal characteristics, thereby refute previous studies that found detrimental effects of Onyx embolization on SRS-induced AVM obliteration. However, given the risks incurred by nidal embolization using Onyx, this neoadjuvant intervention should be used judiciously in multimodal treatment strategies involving SRS for appropriately selected large-volume or angioarchitecturally high-risk AVMs.
关于新辅助Onyx栓塞和立体定向放射外科治疗(SRS)联合治疗脑动静脉畸形(AVM)的研究尚未考虑神经血管内介入治疗前的初始血管构筑特征。这项回顾性、多中心匹配队列研究的目的是利用栓塞前病灶的原始特征,比较接受SRS联合或不联合前期Onyx栓塞治疗AVM的疗效。
回顾性分析国际放射外科研究基金会1987年至2018年的AVM数据库。根据AVM治疗方法将患者分为Onyx栓塞(OE)联合SRS(OE+SRS)组或单纯SRS(仅SRS)组,然后按1:1的比例进行倾向评分匹配。主要结局是AVM闭塞。次要结局包括SRS后出血、全因死亡率、放射学和有症状的放射性改变(RICs)以及囊肿形成。采用粗率和校正死亡竞争风险后的累积概率进行比较分析。
匹配的OE+SRS组和仅SRS组各有53例患者。AVM闭塞的粗率(OE+SRS组与仅SRS组分别为37.7%和47.2%;OR 0.679,p = 0.327)以及3、4、5和6年时的累积概率(OE+SRS组分别为33.7%、44.1%、57.5%和65.7%,仅SRS组分别为34.8%、45.5%、59.0%和67.1%;亚风险比0.961,p = 0.896)在匹配队列中相似。匹配队列的次要结局也相似。匹配的OE+SRS组无症状和有症状的栓塞相关并发症发生率分别为18.9%和9.4%。
SRS前用Onyx进行AVM栓塞似乎不会对SRS后的疗效产生负面影响。基于病灶原始特征的这些分析反驳了之前认为Onyx栓塞对SRS诱导的AVM闭塞有不利影响的研究。然而,鉴于使用Onyx进行病灶栓塞存在风险,在涉及SRS的多模式治疗策略中,对于适当选择的大体积或血管构筑高风险AVM,应谨慎使用这种新辅助干预措施。