Richardson Sarah J, Davis Daniel H J, Stephan Blossom C M, Robinson Louise, Brayne Carol, Barnes Linda E, Taylor John-Paul, Parker Stuart G, Allan Louise M
Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne NE4 5PL, UK.
MRC Unit for Lifelong Health and Ageing at UCL, London WC1E 7HB, UK.
Age Ageing. 2021 May 5;50(3):914-920. doi: 10.1093/ageing/afaa244.
Delirium is common, distressing and associated with poor outcomes. Previous studies investigating the impact of delirium on cognitive outcomes have been limited by incomplete ascertainment of baseline cognition or lack of prospective delirium assessments. This study quantified the association between delirium and cognitive function over time by prospectively ascertaining delirium in a cohort aged ≥ 65 years in whom baseline cognition had previously been established.
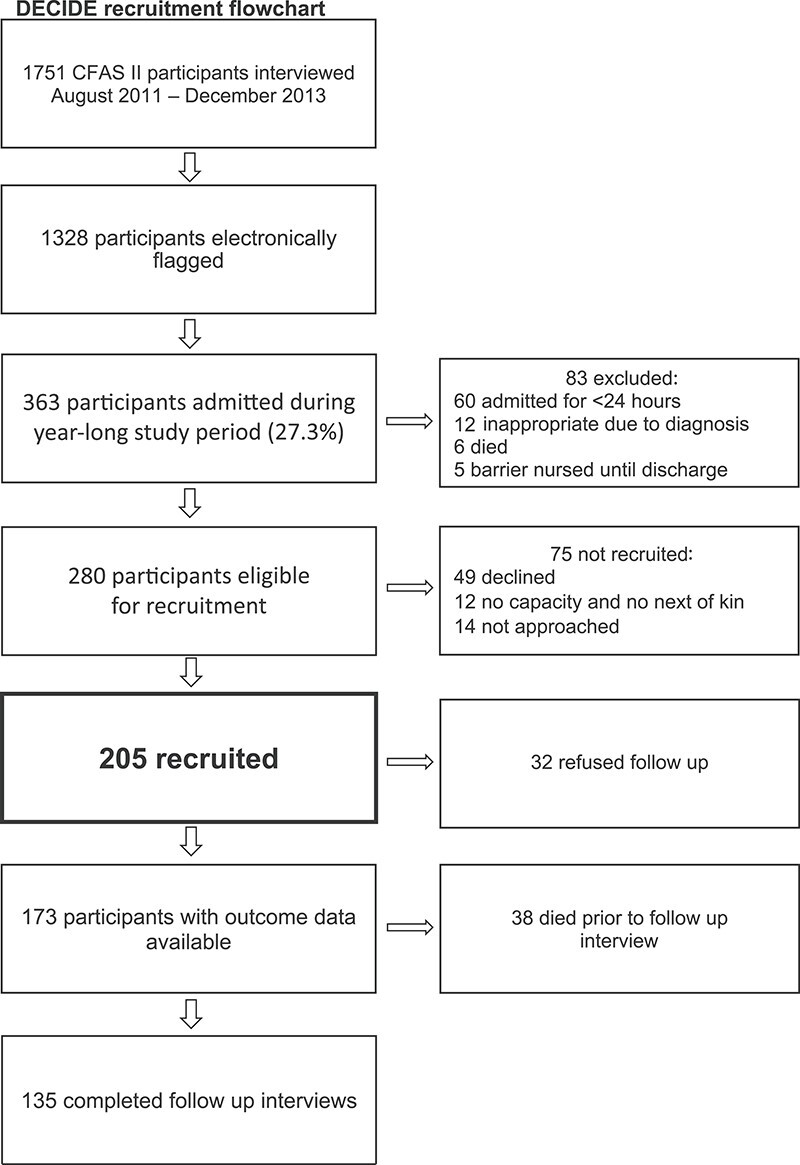
For 12 months, we assessed participants from the Cognitive Function and Ageing Study II-Newcastle for delirium daily during hospital admissions. At 1-year, we assessed cognitive decline and dementia in those with and without delirium. We evaluated the effect of delirium (including its duration and number of episodes) on cognitive function over time, independently of baseline cognition and illness severity.
Eighty two of 205 participants recruited developed delirium in hospital (40%). One-year outcome data were available for 173 participants: 18 had a new dementia diagnosis, 38 had died. Delirium was associated with cognitive decline (-1.8 Mini-Mental State Examination points [95% CI -3.5 to -0.2]) and an increased risk of new dementia diagnosis at follow up (OR 8.8 [95% CI 1.9-41.4]). More than one episode and more days with delirium (>5 days) were associated with worse cognitive outcomes.
Delirium increases risk of future cognitive decline and dementia, independent of illness severity and baseline cognition, with more episodes associated with worse cognitive outcomes. Given that delirium has been shown to be preventable in some cases, we propose that delirium is a potentially modifiable risk factor for dementia.
谵妄很常见,令人痛苦,且与不良预后相关。以往研究谵妄对认知结局影响时,因基线认知确定不完整或缺乏前瞻性谵妄评估而受到限制。本研究通过前瞻性确定≥65岁队列中的谵妄情况,量化了谵妄与认知功能随时间的关联,该队列此前已确定基线认知情况。
在12个月内,我们在医院住院期间每天对认知功能与衰老研究II - 纽卡斯尔的参与者进行谵妄评估。在1年时,我们评估了有谵妄和无谵妄者的认知衰退和痴呆情况。我们评估了谵妄(包括其持续时间和发作次数)随时间对认知功能的影响,独立于基线认知和疾病严重程度。
招募的205名参与者中有82名在医院发生谵妄(40%)。173名参与者有1年结局数据:18名被诊断为新发痴呆,38名死亡。谵妄与认知衰退(简易精神状态检查表降低1.8分[95%置信区间 -3.5至 -0.2])以及随访时新发痴呆诊断风险增加(比值比8.8[95%置信区间1.9 - 41.4])相关。不止一次发作以及谵妄天数超过5天与更差的认知结局相关。
谵妄会增加未来认知衰退和痴呆的风险,独立于疾病严重程度和基线认知,发作次数越多,认知结局越差。鉴于已证明谵妄在某些情况下是可预防的,我们提出谵妄是痴呆的一个潜在可改变风险因素。