Department of Pharmacy, St.Marianna University School of Medicine Hospital, Kawasaki, Japan.
Department of Clinical Oncology, St. Marianna University School of Medicine, Kawasaki, Japan.
BMJ Open. 2020 Dec 17;10(12):e041737. doi: 10.1136/bmjopen-2020-041737.
Dexamethasone (DEX) is administered for multiple days to prevent chemotherapy-induced nausea and vomiting for patients receiving highly emetogenic chemotherapy (HEC); however, its notorious side effects have been widely reported. Although our multicentre randomised double-blind comparative study verified non-inferiority of sparing DEX after day 2 of chemotherapy when combined with neurokinin-1 receptor antagonist (NK1-RA) and palonosetron (Palo) for patients receiving HEC regimen, DEX sparing was not non-inferior in patients receiving cisplatin (CDDP)-based HEC regimens in subgroup analysis. Recently, the efficacy of the addition of olanzapine (OLZ) to standard triple antiemetic therapy on HEC has been demonstrated by several phase III trials. This study aims to confirm non-inferiority of DEX sparing when it is combined with NK-1RA, Palo and OLZ in patients receiving CDDP-based HEC regimens.
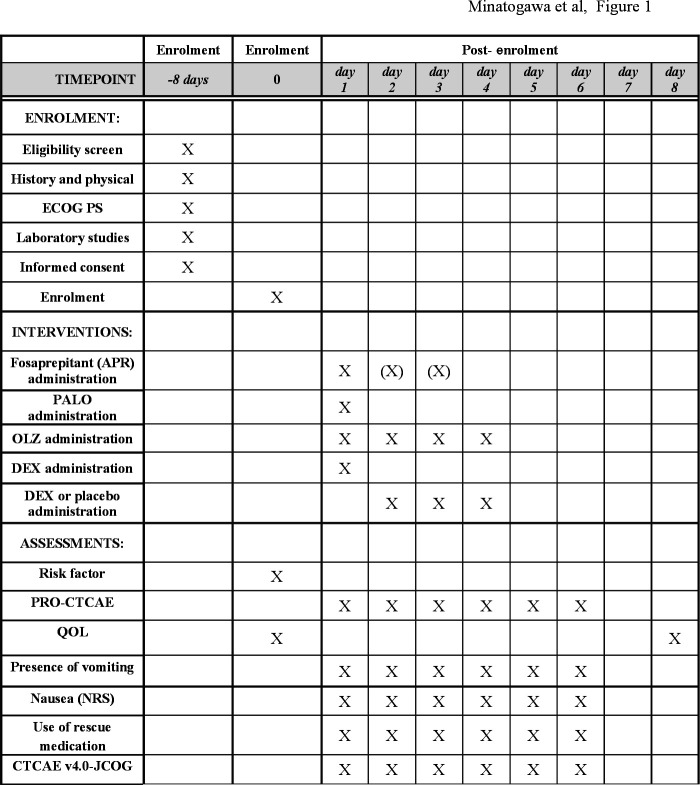
This is a randomised, double-blind, phase III trial. Patients who are scheduled to receive CDDP ≥50 mg/m as initial chemotherapy are eligible. Patients are randomly assigned to receive either DEX on days 1-4 or DEX on day 1 combined with NK1-RA, Palo and OLZ (5 mg). The primary endpoint is complete response (CR) rate, defined as no emesis and no rescue medications during the delayed phase (24-120 hours post-CDDP administration). The non-inferiority margin is set at -15.0%. We assume that CR rates would be 75% in both arms. Two hundred and sixty-two patients are required for at least 80% power to confirm non-inferiority at a one-sided significance level of 2.5%. After considering the possibility of attrition, we set our final required sample size of 280.
The institutional review board approved the study protocol at each of the participating centres. The trial result will be presented at international conferences and published in peer-reviewed journals.
UMIN000032269.
地塞米松(DEX)被用于预防接受高致吐性化疗(HEC)的患者的化疗引起的恶心和呕吐,连续使用数天;然而,其众所周知的副作用已被广泛报道。虽然我们的多中心随机双盲对照研究证实,对于接受 HEC 方案的患者,在化疗第 2 天联合神经激肽-1 受体拮抗剂(NK1-RA)和帕洛诺司琼(Palo)时,节省 DEX 并不劣于第 2 天以后继续使用 DEX,但在亚组分析中,对于接受顺铂(CDDP)为基础的 HEC 方案的患者,节省 DEX 并不劣效。最近,几项 III 期试验证明了奥氮平(OLZ)加入标准三联止吐治疗对 HEC 的疗效。本研究旨在证实 DEX 联合 NK-1RA、Palo 和 OLZ 在接受 CDDP 为基础的 HEC 方案的患者中节省 DEX 的非劣效性。
这是一项随机、双盲、III 期试验。计划接受 CDDP≥50mg/m2 作为初始化疗的患者符合入组条件。患者被随机分配接受 DEX 第 1-4 天或 DEX 第 1 天联合 NK1-RA、Palo 和 OLZ(5mg)。主要终点是完全缓解(CR)率,定义为延迟期(CDDP 给药后 24-120 小时)无呕吐和无解救药物。非劣效性边界设定为-15.0%。我们假设在两组中 CR 率均为 75%。需要 262 名患者,以单侧显著性水平 2.5%达到至少 80%的效力来确认非劣效性。考虑到脱落的可能性后,我们设定了最终需要 280 名患者的样本量。
各参与中心的机构审查委员会批准了研究方案。试验结果将在国际会议上公布,并发表在同行评议的期刊上。
UMIN000032269。