De Cario Rosina, Kura Ada, Suraci Samuele, Magi Alberto, Volta Andrea, Marcucci Rossella, Gori Anna Maria, Pepe Guglielmina, Giusti Betti, Sticchi Elena
Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy.
Department of Information Engineering, University of Florence, Florence, Italy.
Front Genet. 2020 Dec 2;11:592588. doi: 10.3389/fgene.2020.592588. eCollection 2020.
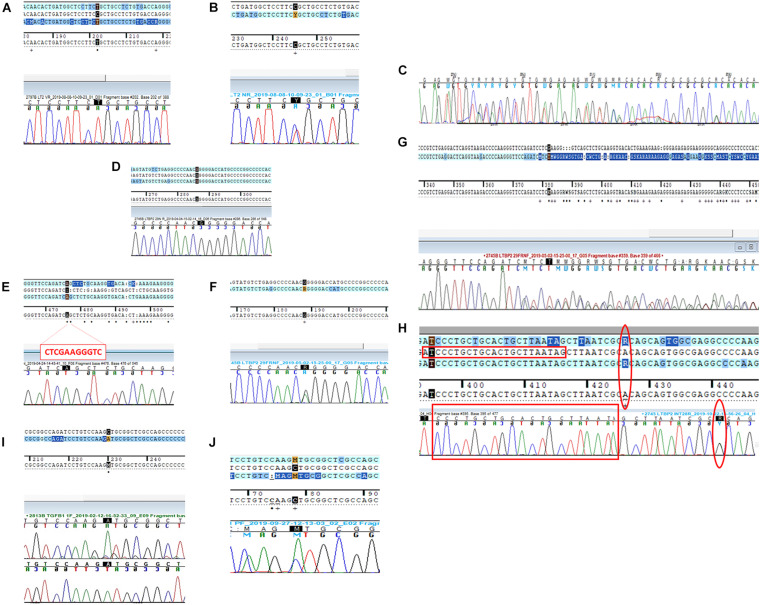
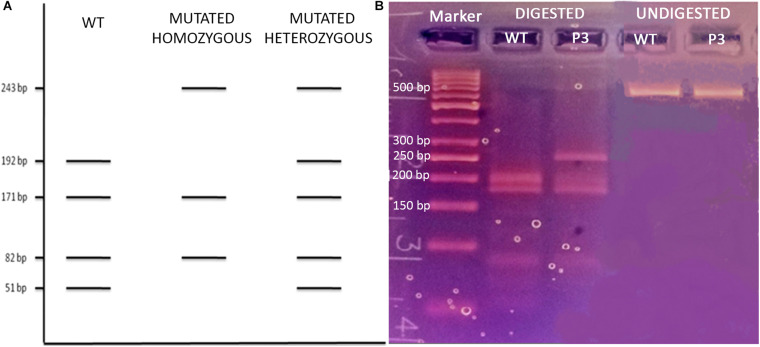
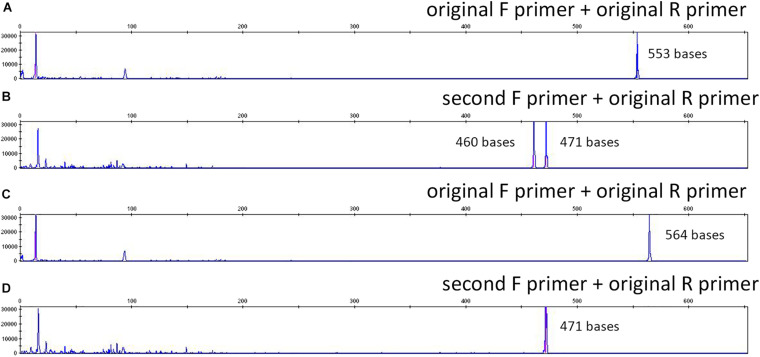
Next-generation sequencing (NGS)'s crucial role in supporting genetic diagnosis and personalized medicine leads to the definition of Guidelines for Diagnostic NGS by the European Society of Human Genetics. Factors of different nature producing false-positive/negative NGS data together with the paucity of internationally accepted guidelines providing specified NGS quality metrics to be followed for diagnostics purpose made the Sanger validation of NGS variants still mandatory. We reported the analysis of three cases of discrepancy between NGS and Sanger sequencing in a cohort of 218 patients. NGS was performed by Illumina MiSeq and Haloplex/SureSelect protocols targeting 97 or 57 or 10 gene panels usually applied for diagnostics. Variants called following guidelines suggested by the Broad Institute and identified according to MAF <0.01 and allele balance >0.2 were Sanger validated. Three out of 945 validated variants showed a discrepancy between NGS and Sanger. In all three cases, a deep evaluation of the discrepant gene variant results and methodological approach allowed to confirm the NGS datum. Allelic dropout (ADO) occurrence during polymerase chain or sequencing reaction was observed, mainly related to incorrect variant zygosity. Our study extends literature data in which almost 100% "high quality" NGS variants are confirmed by Sanger; moreover, it demonstrates that in case of discrepancy between a high-quality NGS variant and Sanger validation, NGS call should not be assumed to represent the source of the error. Actually, difficulties (i.e., ADO, unpredictable presence of private variants on primer-binding regions) of the so-called gold standard direct sequencing should be considered especially in light of the constantly implemented and accurate high-throughput technologies. Our data along with literature raise a discussion on the opportunity to establish a standardized quality threshold by International Guidelines for clinical NGS in order to limit Sanger confirmation to borderline conditions of variant quality parameters and verification of correct gene variant call/patient coupling on a different blood sample aliquot.
新一代测序(NGS)在支持基因诊断和个性化医疗方面的关键作用促使欧洲人类遗传学学会制定了诊断性NGS指南。不同性质的因素会产生假阳性/阴性的NGS数据,同时缺乏国际公认的提供用于诊断目的的特定NGS质量指标的指南,这使得对NGS变异进行桑格验证仍然是必要的。我们报告了在218例患者队列中对3例NGS与桑格测序结果不一致情况的分析。NGS采用Illumina MiSeq和Haloplex/SureSelect方案进行,针对通常用于诊断的97个或57个或10个基因panel。按照布罗德研究所建议的指南调用并根据MAF<0.01和等位基因平衡>0.2鉴定的变异进行了桑格验证。在945个经验证的变异中,有3个显示NGS与桑格测序结果存在差异。在所有3例中,对不一致的基因变异结果和方法学方法进行深入评估后确认了NGS数据。观察到在聚合酶链反应或测序反应过程中发生了等位基因脱扣(ADO),主要与变异的合子性错误有关。我们的研究扩展了文献数据,其中几乎100%的“高质量”NGS变异通过桑格验证得到确认;此外,它表明在高质量NGS变异与桑格验证结果不一致的情况下,不应假定NGS的调用代表错误来源。实际上,尤其是鉴于不断发展且精确的高通量技术,应考虑所谓金标准直接测序的困难(即ADO、引物结合区域上私人变异的不可预测存在)。我们的数据以及文献引发了关于是否有必要通过国际临床NGS指南建立标准化质量阈值的讨论,以便将桑格验证限制在变异质量参数的临界条件以及对不同血样等分样本上正确基因变异调用/患者匹配的验证。