Department of Haematology, Oncology and Palliative Care, Helios Universitätsklinikum Wuppertal, Wuppertal, Germany.
The Faculty of Business and Law, Anglia Ruskin University, Cambridge, United Kingdom.
J Med Internet Res. 2020 Dec 21;22(12):e18655. doi: 10.2196/18655.
Cancer immunotherapy (CIT), as a monotherapy or in combination with chemotherapy, has been shown to extend overall survival in patients with locally advanced or metastatic non-small cell lung cancer (NSCLC). However, patients experience treatment-related symptoms that they are required to recall between hospital visits. Digital patient monitoring and management (DPMM) tools may improve clinical practice by allowing real-time symptom reporting.
This proof-of-concept pilot study assessed patient and health care professional (HCP) adoption of our DPMM tool, which was designed specifically for patients with advanced or metastatic NSCLC treated with CIT, and the tool's impact on clinical care.
Four advisory boards were assembled in order to co-develop a drug- and indication-specific CIT (CIT+) module, based on a generic CIT DPMM tool from Kaiku Health, Helsinki, Finland. A total of 45 patients treated with second-line single-agent CIT (ie, atezolizumab or otherwise) for advanced or metastatic NSCLC, as well as HCPs, whose exact number was decided by the clinics, were recruited from 10 clinics in Germany, Finland, and Switzerland between February and May 2019. All clinics were provided with the Kaiku Health generic CIT DPMM tool, including our CIT+ module. Data on user experience, overall satisfaction, and impact of the tool on clinical practice were collected using anonymized surveys-answers ranged from 1 (low agreement) to 5 (high agreement)-and HCP interviews; surveys and interviews consisted of closed-ended Likert scales and open-ended questions, respectively. The first survey was conducted after 2 months of DPMM use, and a second survey and HCP interviews were conducted at study end (ie, after ≥3 months of DPMM use); only a subgroup of HCPs from each clinic responded to the surveys and interviews. Survey data were analyzed quantitatively; interviews were recorded, transcribed verbatim, and translated into English, where applicable, for coding and qualitative thematic analysis.
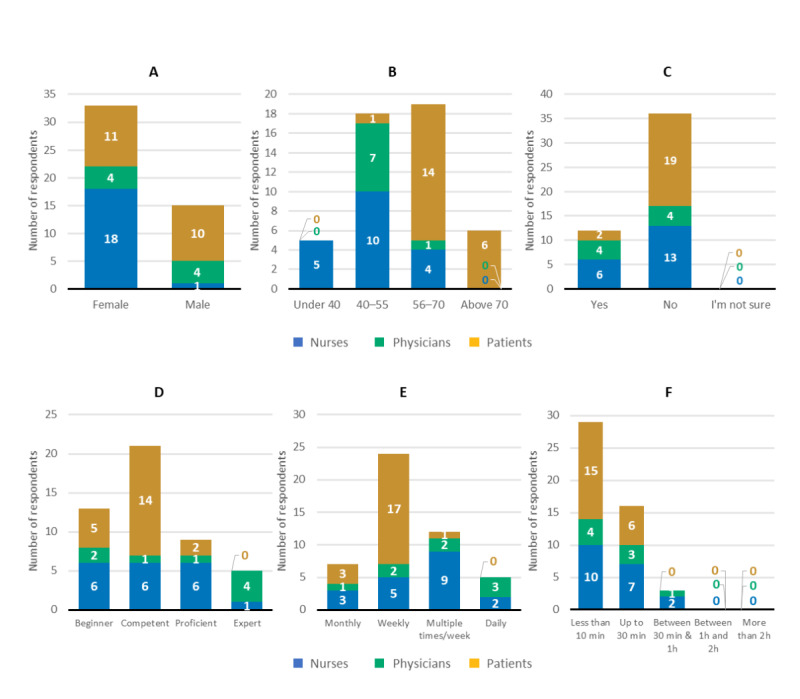
Among interim survey respondents (N=51: 13 [25%] nurses, 11 [22%] physicians, and 27 [53%] patients), mean rankings of the tool's seven usability attributes ranged from 3.2 to 4.4 (nurses), 3.7 to 4.5 (physicians), and 3.7 to 4.2 (patients). At the end-of-study survey (N=48: 19 [40%] nurses, 8 [17%] physicians, and 21 [44%] patients), most respondents agreed that the tool facilitated more efficient and focused discussions between patients and HCPs (nurses and patients: mean rating 4.2, SD 0.8; physicians: mean rating 4.4, SD 0.8) and allowed HCPs to tailor discussions with patients (mean rating 4.35, SD 0.65). The standalone tool was well integrated into HCP daily clinical workflow (mean rating 3.80, SD 0.75), enabled workflow optimization between physicians and nurses (mean rating 3.75, SD 0.80), and saved time by decreasing phone consultations (mean rating 3.75, SD 1.00) and patient visits (mean rating 3.45, SD 1.20). Workload was the most common challenge of tool use among respondents (12/19, 63%).
Our results demonstrate high user satisfaction and acceptance of DPMM tools by HCPs and patients, and highlight the improvements to clinical care in patients with advanced or metastatic NSCLC treated with CIT monotherapy. However, further integration of the tool into the clinical information technology data flow is required. Future studies or registries using our DPMM tool may provide insights into significant effects on patient quality of life or health-economic benefits.
癌症免疫疗法(CIT)作为单一疗法或与化疗联合使用,已被证明可以延长局部晚期或转移性非小细胞肺癌(NSCLC)患者的总生存期。然而,患者在医院就诊之间需要回忆与治疗相关的症状。数字患者监测和管理(DPMM)工具可以通过允许实时症状报告来改善临床实践。
本概念验证性试点研究评估了我们专门为接受 CIT 治疗的晚期或转移性 NSCLC 患者设计的 DPMM 工具的患者和医疗保健专业人员(HCP)的采用情况,以及该工具对临床护理的影响。
为了共同开发一种针对特定药物和适应症的 CIT(CIT+)模块,我们组建了四个顾问委员会,该模块基于来自芬兰赫尔辛基的 Kaiku Health 的通用 CIT DPMM 工具。共有 45 名接受二线单药 CIT(即阿特珠单抗或其他药物)治疗的晚期或转移性 NSCLC 患者以及 HCP(确切人数由诊所决定)于 2019 年 2 月至 5 月期间从德国、芬兰和瑞士的 10 家诊所招募。每家诊所都配备了 Kaiku Health 通用 CIT DPMM 工具,包括我们的 CIT+模块。使用匿名调查收集了有关用户体验、总体满意度和工具对临床实践影响的数据,答案范围为 1(低同意)至 5(高同意),并对 HCP 进行了采访;调查和访谈分别由封闭式李克特量表和开放式问题组成。在 DPMM 使用 2 个月后进行了第一次调查,在研究结束时(即 DPMM 使用≥3 个月后)进行了第二次调查和 HCP 访谈;只有每家诊所的一小部分 HCP 对调查和访谈做出了回应。调查数据进行了定量分析;访谈进行了记录,逐字转录,并翻译为英文,以进行编码和定性主题分析。
在中期调查的应答者中(N=51:13 [25%]护士、11 [22%]医生和 27 [53%]患者),工具的七个可用性属性的平均排名范围为 3.2 至 4.4(护士)、3.7 至 4.5(医生)和 3.7 至 4.2(患者)。在结束时的研究调查中(N=48:19 [40%]护士、8 [17%]医生和 21 [44%]患者),大多数受访者同意该工具促进了患者和 HCP 之间更有效和更有针对性的讨论(护士和患者:平均评分 4.2,SD 0.8;医生:平均评分 4.4,SD 0.8),并允许 HCP 与患者进行个性化讨论(平均评分 4.35,SD 0.65)。独立工具很好地集成到了 HCP 的日常临床工作流程中(平均评分 3.80,SD 0.75),优化了医生和护士之间的工作流程(平均评分 3.75,SD 0.80),并通过减少电话咨询(平均评分 3.75,SD 1.00)和患者就诊(平均评分 3.45,SD 1.20)来节省时间。受访者中最常见的工具使用挑战是工作量(12/19,63%)。
我们的研究结果表明,HCP 和患者对 DPMM 工具的满意度和接受度很高,并强调了在接受 CIT 单一疗法治疗的晚期或转移性 NSCLC 患者中改善了临床护理。然而,需要进一步将该工具集成到临床信息技术数据流中。未来使用我们的 DPMM 工具的研究或注册可能会提供有关对患者生活质量或健康经济效益的重大影响的见解。