Department of Otorhinolaryngology, Head and Neck Surgery, Medical University Vienna, Vienna, Austria.
Center for Medical Statistics, Informatics, and Intelligent Systems, Medical University of Vienna, Vienna, Austria.
Eur Arch Otorhinolaryngol. 2021 Sep;278(9):3479-3488. doi: 10.1007/s00405-020-06541-3. Epub 2020 Dec 21.
To evaluate the impact of tracheostomy on complications, dysphagia and outcome in second and third degree burned patients.
Inpatient mortality, dysphagia, severity of burn injury (ABSI, TBSA) and complications in tracheotomized burn patients were compared to (I) non-tracheotomized burn patients and (II) matched tracheotomized non-burn patients.
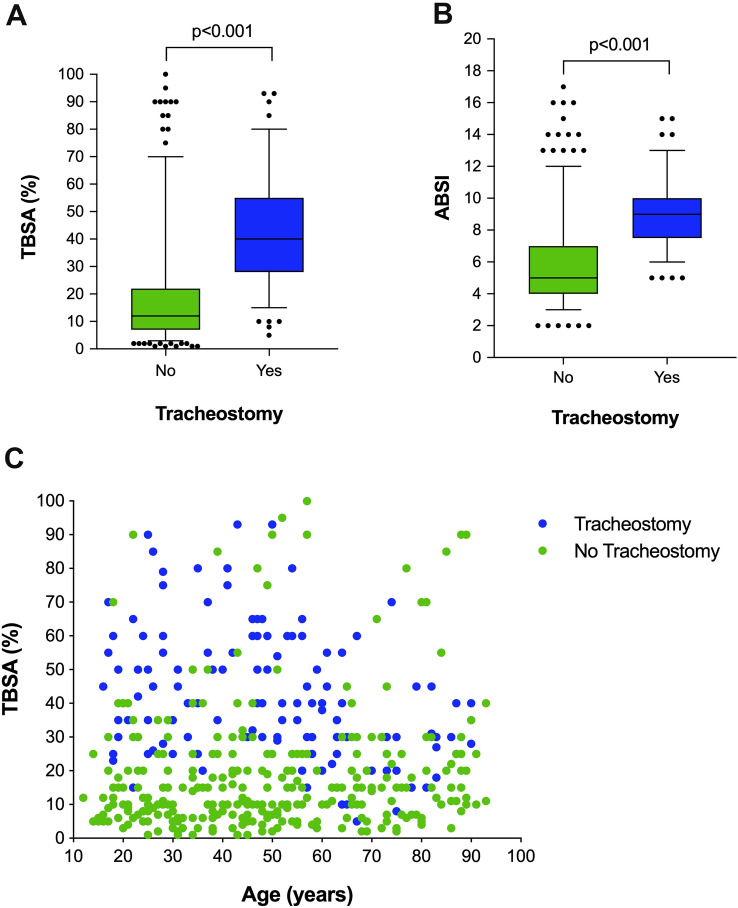
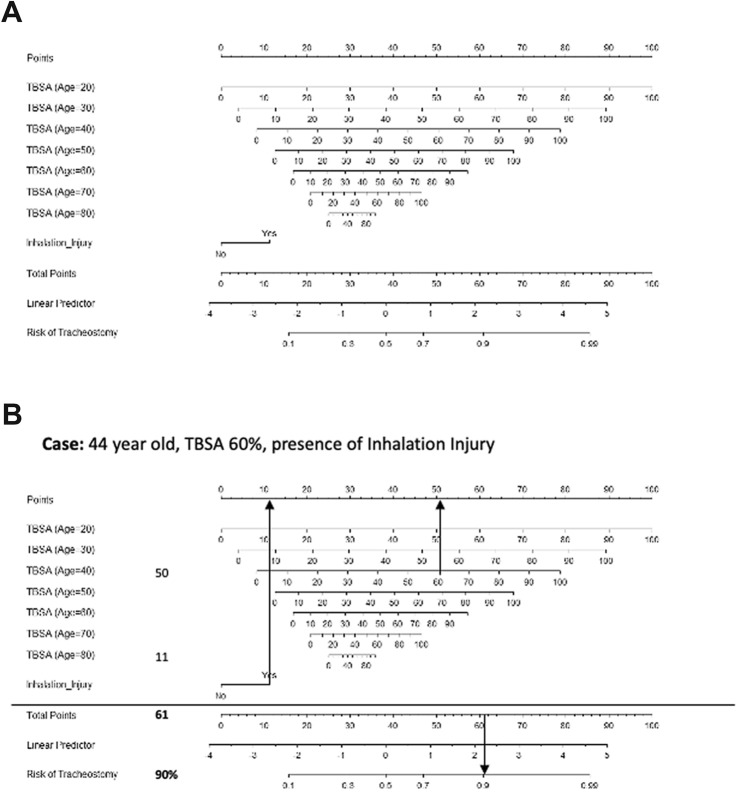
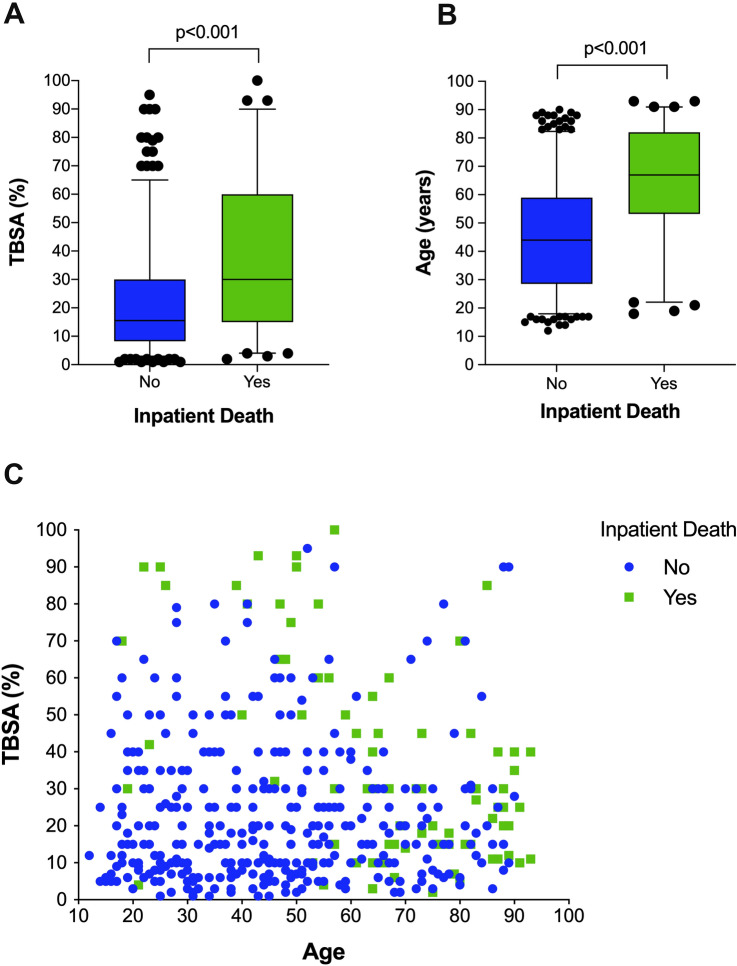
134 (30.9%) out of 433 patients who underwent tracheostomy, had a significantly higher percentage of inhalation injury (26.1% vs. 7.0%; p < 0.001), higher ABSI (8.9 ± 2.1 vs. 6.0 ± 2.7; p < 0.001) and TBSA score (41.4 ± 19.7% vs. 18.6 ± 18.8%; p < 0.001) compared to 299 non-tracheotomized burn patients. However, complications occurred equally in tracheotomized burn patients and matched controls and tracheostomy was neither linked to dysphagia nor to inpatient mortality at multivariate analysis. In particular, dysphagia occurred in 6.2% of cases and was significantly linked to length of ICU stay (OR 6.2; p = 0.021), preexisting neurocognitive impairments (OR 5.2; p = 0.001) and patients' age (OR 3.4; p = 0.046). A nomogram was calculated based on age, TBSA and inhalation injury predicting the need for a tracheostomy in severely burned patients.
Using the new nomogram we were able to predict with significantly higher accuracy the need for tracheostomy in severely burned patients. Moreover, tracheostomy is safe and is not associated with higher incidenc of complications, dysphagia or worse outcome.
评估气管切开术对二度和三度烧伤患者并发症、吞咽困难和结局的影响。
比较气管切开的烧伤患者与(I)非气管切开的烧伤患者和(II)匹配的气管切开的非烧伤患者的住院死亡率、吞咽困难、烧伤严重程度(ABSI、TBSA)和并发症。
在 433 例行气管切开术的患者中,有 134 例(30.9%)有明显更高的吸入性损伤比例(26.1%比 7.0%;p<0.001)、更高的 ABSI(8.9±2.1 比 6.0±2.7;p<0.001)和 TBSA 评分(41.4±19.7%比 18.6±18.8%;p<0.001),与 299 例非气管切开的烧伤患者相比。然而,气管切开的烧伤患者与匹配的对照组的并发症发生率相同,并且多变量分析显示气管切开术与吞咽困难或住院死亡率无关。特别是,吞咽困难的发生率为 6.2%,与 ICU 住院时间(OR 6.2;p=0.021)、预先存在的神经认知障碍(OR 5.2;p=0.001)和患者年龄(OR 3.4;p=0.046)显著相关。基于年龄、TBSA 和吸入性损伤,我们计算了一个列线图来预测严重烧伤患者需要气管切开术。
使用新的列线图,我们能够更准确地预测严重烧伤患者需要气管切开术的情况。此外,气管切开术是安全的,与并发症、吞咽困难或更差的结局发生率增加无关。