Department of Hematology.
Department of Endocrinology.
Blood Adv. 2020 Dec 22;4(24):6353-6363. doi: 10.1182/bloodadvances.2020003323.
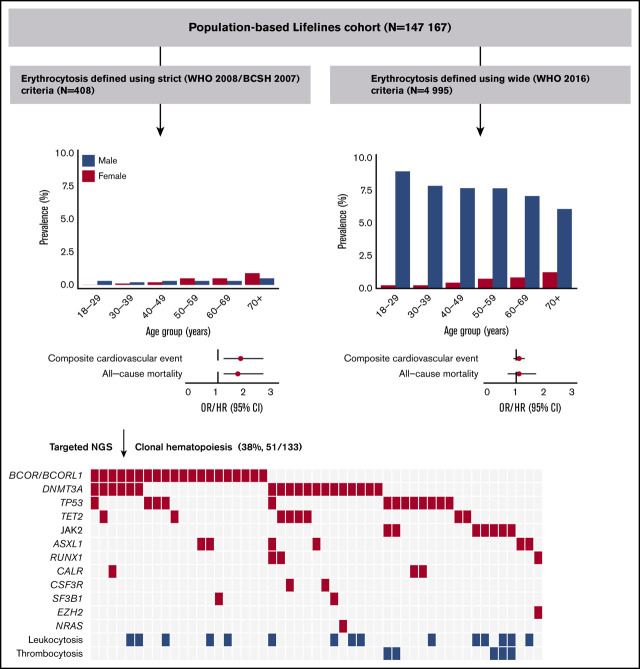
Erythrocytosis is a common reason for referral to hematology services and is usually secondary in origin. The aim of this study was to assess clinical characteristics and clonal hematopoiesis (CH) in individuals with erythrocytosis in the population-based Lifelines cohort (n = 147 167). Erythrocytosis was defined using strict (World Health Organization [WHO] 2008/British Committee for Standards in Hematology) and wide (WHO 2016) criteria. Individuals with erythrocytosis (strict criteria) and concurrent leukocytosis and/or thrombocytosis were 1:2 matched with individuals with isolated erythrocytosis and analyzed for somatic mutations indicative of CH (≥5% variant allele frequency). One hundred eighty five males (0.3%) and 223 females (0.3%) met the strict criteria, whereas 4868 males (7.6%) and 309 females (0.4%) met the wide criteria. Erythrocytosis, only when defined using strict criteria, was associated with cardiovascular morbidity (odds ratio [OR], 1.8; 95% confidence interval [CI], 1.2-2.6), cardiovascular mortality (hazard ratio [HR], 2.2; 95% CI, 1.0-4.6), and all-cause mortality (HR, 1.7; 95% CI, 1.2-2.6), independent of conventional risk factors. Mutations were detected in 51 of 133 (38%) evaluable individuals, with comparable frequencies between individuals with and without concurrent cytosis. The JAK2 V617F mutation was observed in 7 of 133 (5.3%) individuals, all having concurrent cytosis. The prevalence of mutations in BCOR/BCORL1 (16%) was high, suggesting aberrant epigenetic regulation. Erythrocytosis with CH was associated with cardiovascular morbidity (OR, 9.1; 95% CI, 1.2-68.4) in a multivariable model. Our data indicate that only when defined using strict criteria erythrocytosis is associated with cardiovascular morbidity (especially in the presence of CH), cardiovascular mortality, and all-cause mortality.
红细胞增多症是向血液科就诊的常见原因,通常是继发的。本研究旨在评估基于人群的 Lifelines 队列(n=147167)中红细胞增多症患者的临床特征和克隆性造血(CH)。红细胞增多症采用严格(世界卫生组织[WHO]2008/英国血液学标准委员会)和广泛(WHO 2016)标准定义。用严格标准(WHO 2008/英国血液学标准委员会)定义的红细胞增多症伴白细胞增多和/或血小板增多的患者与单纯红细胞增多症患者按 1:2 配对,并分析提示 CH 的体细胞突变(≥5%变异等位基因频率)。185 名男性(0.3%)和 223 名女性(0.3%)符合严格标准,而 4868 名男性(7.6%)和 309 名女性(0.4%)符合广泛标准。只有当使用严格标准定义红细胞增多症时,与心血管发病率(比值比[OR],1.8;95%置信区间[CI],1.2-2.6)、心血管死亡率(风险比[HR],2.2;95%CI,1.0-4.6)和全因死亡率(HR,1.7;95%CI,1.2-2.6)相关,独立于传统危险因素。在 133 名可评估患者中,有 51 名(38%)检测到突变,伴有或不伴有伴发性细胞增多症的患者突变频率相似。JAK2 V617F 突变在 133 名患者中的 7 名(5.3%)中被发现,所有患者均伴有伴发性细胞增多症。BCOR/BCORL1 突变(16%)的发生率较高,提示存在异常的表观遗传调控。在多变量模型中,伴有 CH 的红细胞增多症与心血管发病率(OR,9.1;95%CI,1.2-68.4)相关。我们的数据表明,只有当使用严格标准定义红细胞增多症时,才与心血管发病率(特别是在伴有 CH 时)、心血管死亡率和全因死亡率相关。