Gresser Eva, Rueckel Johannes, Puhr-Westerheide Daniel, Schwarze Vincent, Fink Nicola, Kunz Wolfgang G, Wassilowsky Dietmar, Irlbeck Michael, Ricke Jens, Ingrisch Michael, Sabel Bastian O
Department of Radiology, University Hospital, LMU Munich, 81377 Munich, Germany.
Department of Anaesthesiology, University Hospital, LMU Munich, 81377 Munich, Germany.
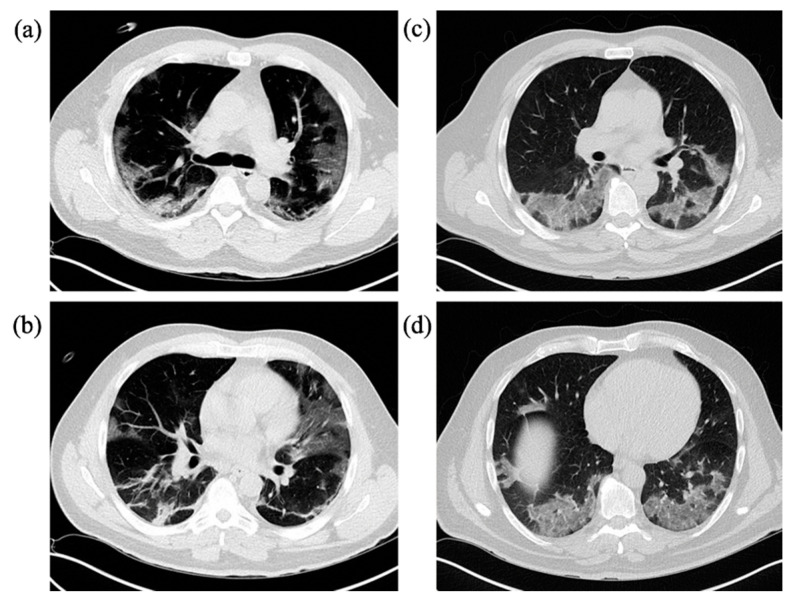
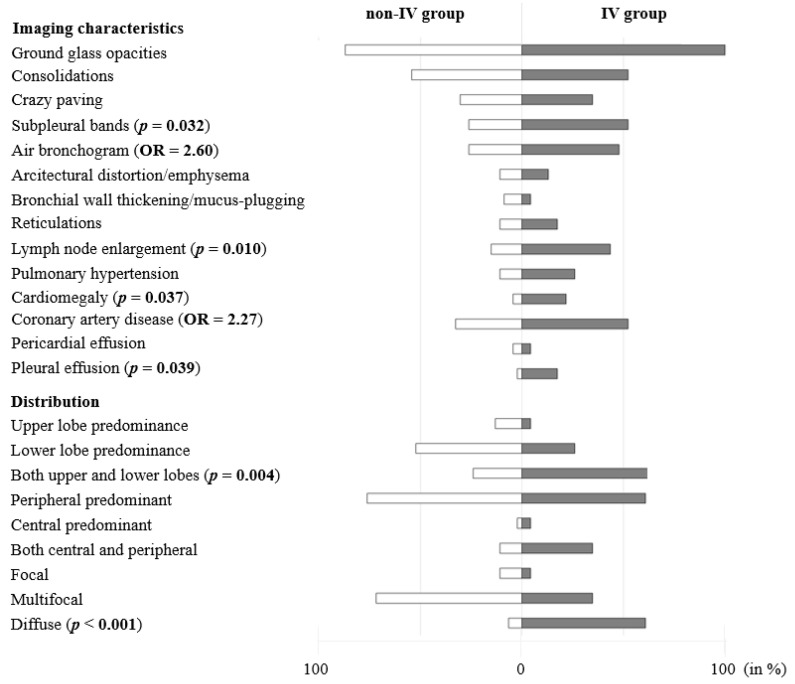
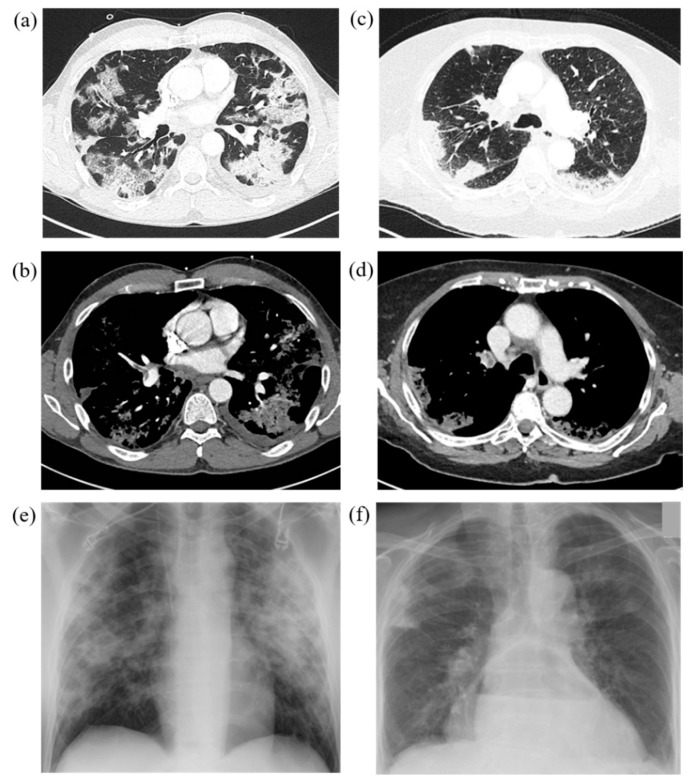
Diagnostics (Basel). 2020 Dec 19;10(12):1108. doi: 10.3390/diagnostics10121108.
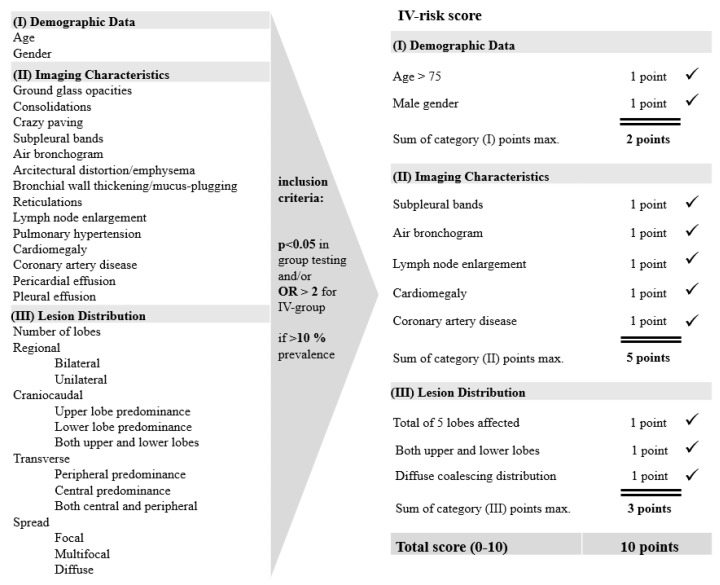
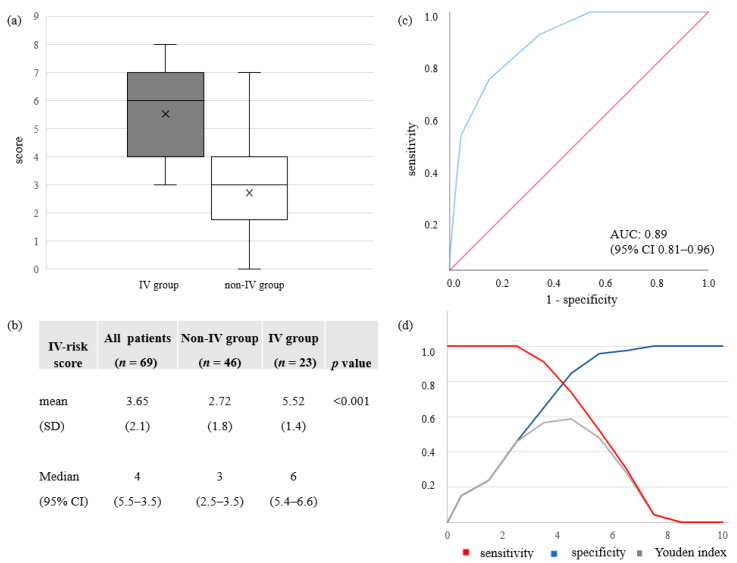
(1) Background: To assess the value of chest CT imaging features of COVID-19 disease upon hospital admission for risk stratification of invasive ventilation (IV) versus no or non-invasive ventilation (non-IV) during hospital stay. (2) Methods: A retrospective single-center study was conducted including all patients admitted during the first three months of the pandemic at our hospital with PCR-confirmed COVID-19 disease and admission chest CT scans ( = 69). Using clinical information and CT imaging features, a 10-point ordinal risk score was developed and its diagnostic potential to differentiate a severe (IV-group) from a more moderate course (non-IV-group) of the disease was tested. (3) Results: Frequent imaging findings of COVID-19 pneumonia in both groups were ground glass opacities (91.3%), consolidations (53.6%) and crazy paving patterns (31.9%). Characteristics of later stages such as subpleural bands were observed significantly more often in the IV-group (52.2% versus 26.1%, = 0.032). Using information directly accessible during a radiologist's reporting, a simple risk score proved to reliably differentiate between IV- and non-IV-groups (AUC: 0.89 (95% CI 0.81-0.96), < 0.001). (4) Conclusions: Information accessible from admission CT scans can effectively and reliably be used in a scoring model to support risk stratification of COVID-19 patients to improve resource and allocation management of hospitals.
(1)背景:评估新冠病毒病(COVID-19)入院时胸部CT影像特征对住院期间有创通气(IV)与无创通气或不进行通气(非IV)风险分层的价值。(2)方法:进行一项回顾性单中心研究,纳入在我院疫情爆发的前三个月期间收治的所有经PCR确诊为COVID-19且有入院胸部CT扫描的患者(n = 69)。利用临床信息和CT影像特征,制定了一个10分的序贯风险评分,并测试其区分疾病严重病程(IV组)和较中度病程(非IV组)的诊断潜力。(3)结果:两组中COVID-19肺炎常见的影像表现为磨玻璃影(91.3%)、实变(53.6%)和铺路石样改变(31.9%)。IV组中观察到更多后期特征,如胸膜下条索影(52.2%对26.1%,P = 0.032)。利用放射科医生报告时可直接获取的信息,一个简单的风险评分被证明能可靠地区分IV组和非IV组(AUC:0.89(95%CI 0.81 - 0.96),P < 0.001)。(4)结论:入院CT扫描获得的信息可有效且可靠地用于评分模型,以支持COVID-19患者的风险分层,改善医院的资源和分配管理。