Olsen Markus Harboe, Møller Marcus, Romano Stefano, Andersson Jonas, Mlodzinski Eric, Raines Nathan H, Sherak Raphael, Jeppesen Anni Nørgaard
Department of Neuroanaesthesiology, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark.
Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark.
Crit Care Explor. 2020 Dec 16;2(12):e0304. doi: 10.1097/CCE.0000000000000304. eCollection 2020 Dec.
Describe the relationship between ICU-acquired hypernatremia and in-hospital mortality and investigate the optimal hypernatremia correction rate.
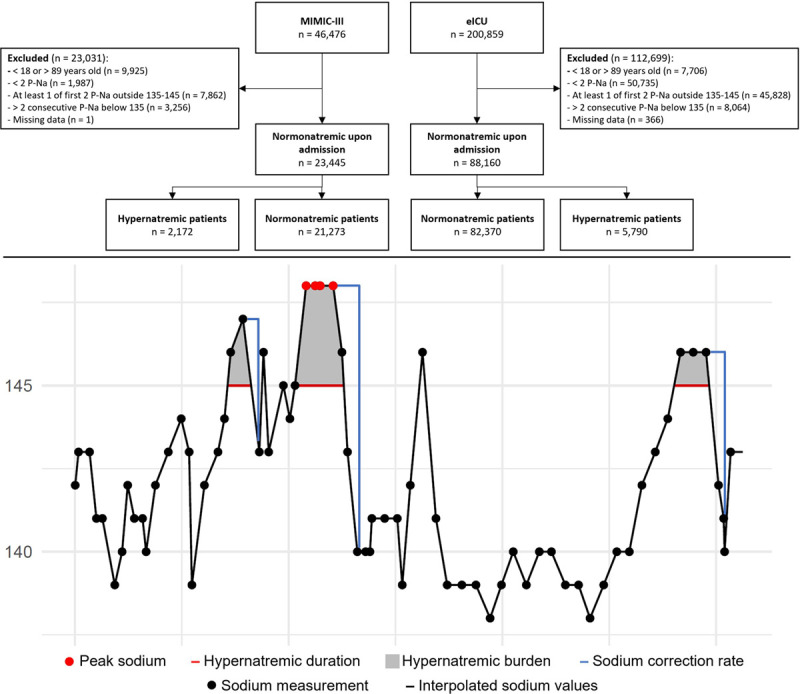
Observational study including two individual ICU cohorts. We used the Medical Information Mart for Intensive Care III v. 1.4 database consists of all ICU patients admitted to the Beth Israel Deaconess Medical Center in Boston from 2001 to 2012 ( = 46,476). The electronic ICU v. 2.0 database consists of all ICU patients admitted to 208 distinct hospitals across the United States from 2014 to 2015 ( = 200,859). We included all adult patients admitted to an ICU with two consecutive sodium samples within normal range (135-145 mmol/L) and without two consecutive hyponatremic samples (< 135 mmol/L) during the ICU stay.
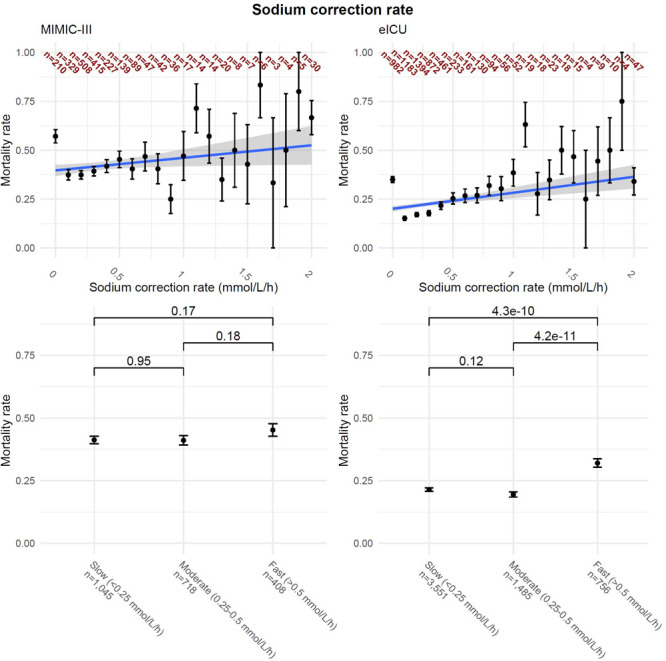
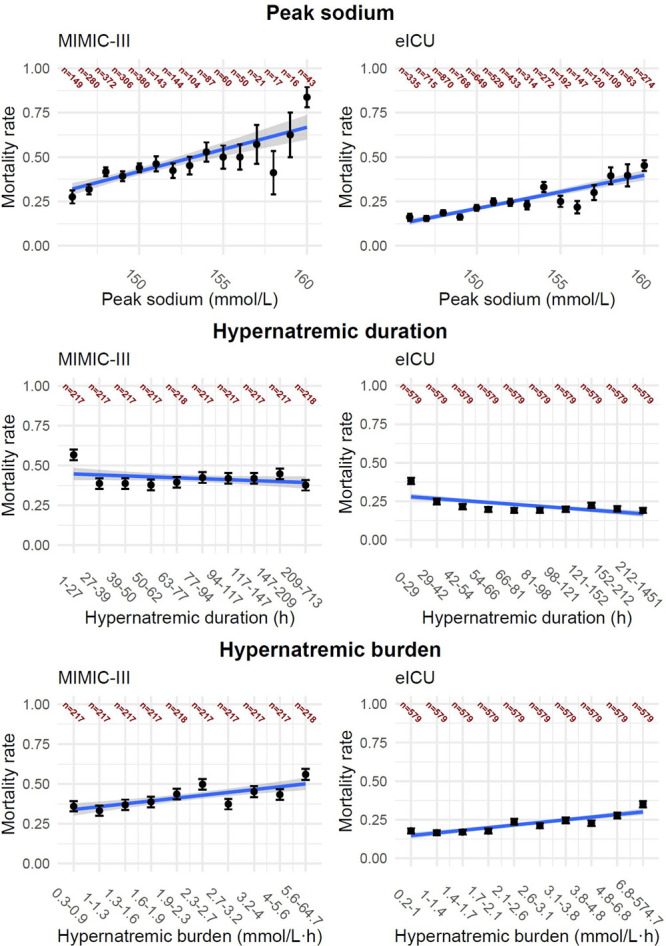
Of 23,445 patients identified in Medical Information Mart for Intensive Care III, 9% ( = 2,172) developed hypernatremia during their ICU stay. In electronic ICU, 88,160 patients were identified and 7% ( = 5,790) developed hypernatremia. In both cohorts, patients with hypernatremia had a higher mortality (Medical Information Mart for Intensive Care III: 20% vs 42%; < 0.01 and electronic ICU: 6% vs 22%; < 0.01), with hypernatremia increasing the risk of in-hospital mortality (Medical Information Mart for Intensive Care III: odds ratio, 1.15; 95% CI, 1.13-1.17 and electronic ICU: odds ratio, 1.11; 95% CI, 1.10-1.12) and over time using a Cox regression. Rapid sodium correction rate (> 0.5 mmol/L/hr) was associated with an increased in-hospital mortality in both cohorts (Medical Information Mart for Intensive Care III: odds ratio, 1.08; 95% CI, 1.03-1.13 and electronic ICU: odds ratio, 1.10; 95% CI, 1.06-1.13). In the electronic ICU cohort, rapid correction rates were associated with a significant difference in in-hospital mortality, but there was no statistically significant association in the Medical Information Mart for Intensive Care III cohort.
ICU-acquired hypernatremia is associated with increased in-hospital mortality. Furthermore, a rapid sodium correction rates may be harmful. This suggests it is important to both prevent ICU-acquired hypernatremia and to avoid rapid correction rates if a patient becomes hypernatremic.
描述重症监护病房获得性高钠血症与院内死亡率之间的关系,并研究最佳的高钠血症纠正率。
设计、地点、参与者和测量方法:观察性研究,包括两个独立的重症监护病房队列。我们使用重症监护医学信息集市III版1.4数据库,该数据库包含2001年至2012年在波士顿贝斯以色列女执事医疗中心收治的所有重症监护病房患者(n = 46,476)。电子重症监护病房2.0数据库包含2014年至2015年在美国208家不同医院收治的所有重症监护病房患者(n = 200,859)。我们纳入了所有入住重症监护病房的成年患者,这些患者在重症监护病房住院期间有两个连续的钠样本在正常范围内(135 - 145 mmol/L),且没有两个连续的低钠血症样本(< 135 mmol/L)。
在重症监护医学信息集市III中识别出的23,445例患者中,9%(n = 2,172)在重症监护病房住院期间发生高钠血症。在电子重症监护病房中识别出88,160例患者,7%(n = 5,790)发生高钠血症。在两个队列中,高钠血症患者的死亡率更高(重症监护医学信息集市III:20%对42%;P < 0.01,电子重症监护病房:6%对22%;P < 0.01),高钠血症增加了院内死亡风险(重症监护医学信息集市III:比值比,1.15;95%置信区间,1.13 - 1.17,电子重症监护病房:比值比,1.11;95%置信区间,1.10 - 1.12),并通过Cox回归分析随时间变化的情况。快速钠纠正率(> 0.5 mmol/L/小时)与两个队列的院内死亡率增加相关(重症监护医学信息集市III:比值比,1.08;95%置信区间,1.03 - 1.13,电子重症监护病房:比值比,1.10;95%置信区间,1.06 - 1.13)。在电子重症监护病房队列中,快速纠正率与院内死亡率存在显著差异,但在重症监护医学信息集市III队列中没有统计学上的显著关联。
重症监护病房获得性高钠血症与院内死亡率增加相关。此外,快速的钠纠正率可能有害。这表明预防重症监护病房获得性高钠血症以及如果患者发生高钠血症时避免快速纠正率都很重要。