Zhang Li-Peng, Ren Hu, Du Yong-Xing, Wang Cheng-Feng
Department of Pancreatic and Gastric Surgery, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, China.
World J Gastroenterol. 2020 Dec 14;26(46):7382-7404. doi: 10.3748/wjg.v26.i46.7382.
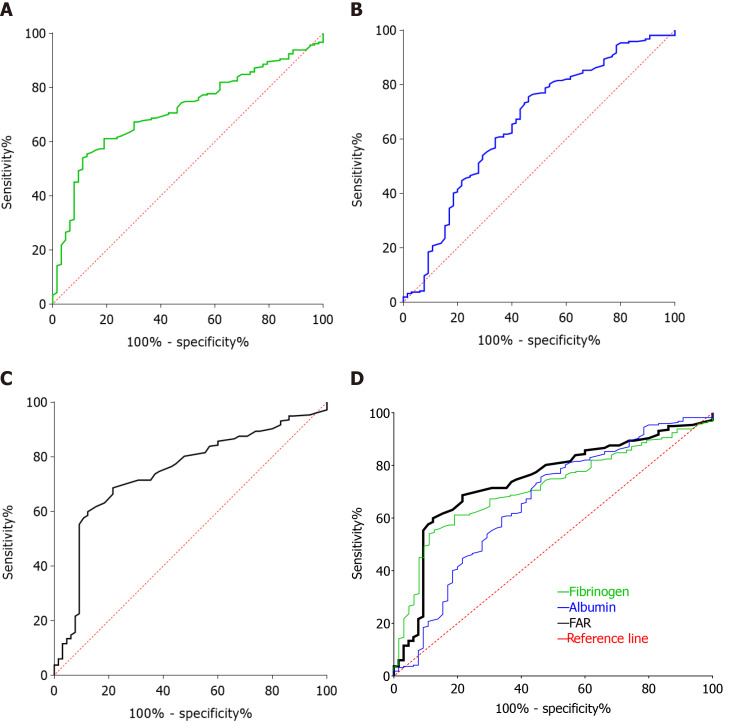
Inflammation plays an important role in tumor progression, and growing evidence has confirmed that the fibrinogen-to-albumin ratio (FAR) is an important prognostic factor for overall survival in malignant tumors.
To investigate the prognostic significance of FAR in patients undergoing radical R0 resection of pancreatic ductal adenocarcinoma (PDAC).
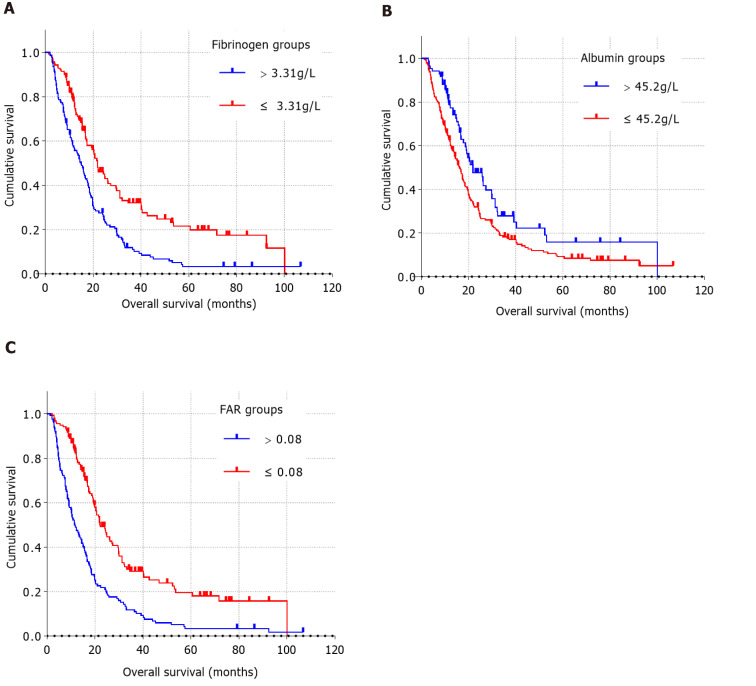
We retrospectively analyzed the data of 282 patients with PDAC who underwent radical R0 resection at The Cancer Hospital of the Chinese Academy of Medical Sciences from January 2010 to December 2019. The surv_cutpoint function of the R package survminer RStudio software (version 1.3.1073, http://www.rstudio.org) was used to determine the optimal cut-off values of biological markers, such as preoperative FAR. The Kaplan-Meier method and log-rank tests were used for univariate survival analysis, and a Cox regression model was used for multivariate survival analysis for PDAC patients who underwent radical R0 resection.
The optimal cut-off value of FAR was 0.08 by the surv_cutpoint function. Higher preoperative FAR was significantly correlated with clinical symptoms ( = 0.001), tumor location ( < 0.001), surgical approaches ( < 0.001), preoperative plasma fibrinogen concentration ( < 0.001), and preoperative plasma albumin level ( < 0.001). Multivariate analysis showed that degree of tumor differentiation ( < 0.001), number of metastatic lymph nodes [hazard ratio (HR): 0.678, 95% confidence interval (CI): 0.509-0.904, = 0.008], adjuvant therapy (HR: 1.604, 95%CI: 1.214-2.118, = 0.001), preoperative cancer antigen 19-9 level (HR: 1.740, 95%CI: 1.288-2.352, < 0.001), and preoperative FAR (HR: 2.258, 95%CI: 1.720-2.963, < 0.001) were independent risk factors for poor prognosis in patients with PDAC who underwent radical R0 resection.
The increase in preoperative FAR was significantly related to poor prognosis in patients undergoing radical R0 resection for PDAC. Preoperative FAR can be used clinically to predict the prognosis of PDAC patients undergoing radical R0 resection.
炎症在肿瘤进展中起重要作用,越来越多的证据证实纤维蛋白原与白蛋白比值(FAR)是恶性肿瘤总生存期的重要预后因素。
探讨FAR在接受胰腺导管腺癌(PDAC)根治性R0切除患者中的预后意义。
我们回顾性分析了2010年1月至2019年12月在中国医学科学院肿瘤医院接受根治性R0切除的282例PDAC患者的数据。使用R包survminer RStudio软件(版本1.3.1073,http://www.rstudio.org)的surv_cutpoint函数确定生物标志物(如术前FAR)的最佳临界值。采用Kaplan-Meier法和对数秩检验进行单因素生存分析,采用Cox回归模型对接受根治性R0切除的PDAC患者进行多因素生存分析。
通过surv_cutpoint函数确定FAR的最佳临界值为0.08。术前FAR较高与临床症状(P = 0.001)、肿瘤位置(P < 0.001)、手术方式(P < 0.001)、术前血浆纤维蛋白原浓度(P < 0.001)及术前血浆白蛋白水平(P < 0.001)显著相关。多因素分析显示,肿瘤分化程度(P < 0.001)、转移淋巴结数量[风险比(HR):0.678,95%置信区间(CI):0.509 - 0.904,P = 0.008]、辅助治疗(HR:1.604,95%CI:1.214 - 2.118,P = 0.001)、术前癌抗原19 - 9水平(HR:1.740,95%CI:1.288 - 2.352,P < 0.001)及术前FAR(HR:2.258,95%CI:1.720 - 2.963,P < 0.001)是接受根治性R0切除的PDAC患者预后不良的独立危险因素。
术前FAR升高与接受PDAC根治性R0切除患者的不良预后显著相关。术前FAR可在临床上用于预测接受根治性R0切除的PDAC患者的预后。