Department of Gastrointestinal Medical Oncology, Harbin Medical University Cancer Hospital, Harbin, China.
Translational Medicine Research and Cooperation Center of Northern China, Heilongjiang Academy of Medical Sciences, Harbin, China.
Cancer Res Treat. 2021 Jan;53(1):131-139. doi: 10.4143/crt.2020.330. Epub 2020 Aug 24.
Systemic inflammatory response is a critical factor that promotes the initiation and metastasis of malignancies including pancreatic cancer (PC). This study was designed to determine and compare the prognostic value of neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), and fibrinogen-to-albumin ratio (FAR) in resectable PC and locally advanced or metastatic PC.
Three hundred fifty-three patients with resectable PC and 807 patients with locally advan-ced or metastatic PC were recruited in this study. These patients were classified into a training set (n=758) and a validation set (n=402). Kaplan-Meier survival plots and Cox proportional hazards regression models were used to analyze prognosis.
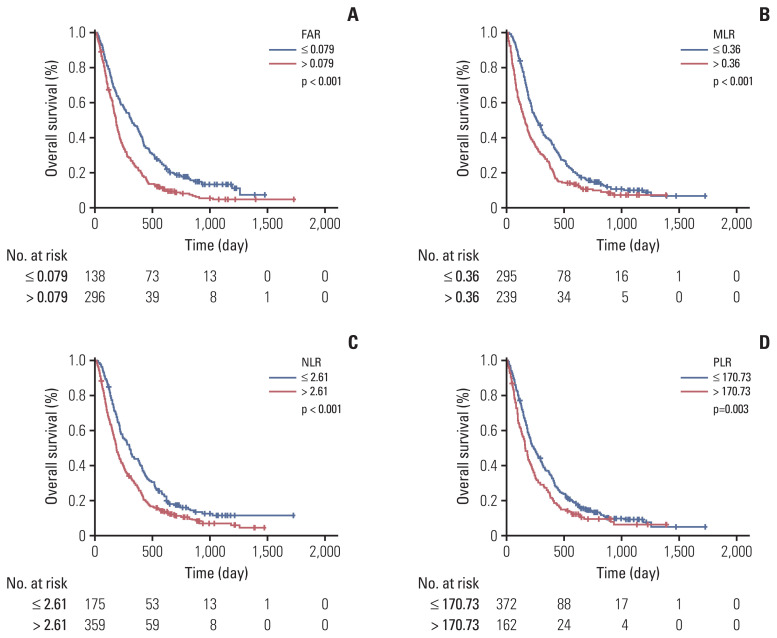
Overall survival (OS) was significantly better for patients with resectable PC with low preoperative PLR (p=0.048) and MLR (p=0.027). Low FAR, MLR, NLR (p < 0.001), and PLR (p=0.003) were significantly associated with decreased risk of death for locally advanced or metastatic PC patients. FAR (hazard ratio [HR], 1.522; 95% confidential interval [CI], 1.261 to 1.837; p < 0.001) and MLR (HR, 1.248; 95% CI, 1.017 to 1.532; p=0.034) were independent prognostic factors for locally advanced or metastatic PC.
The prognostic roles of FAR, MLR, NLR, and PLR in resectable PC and locally advanced or metastatic PC were different. FAR showed the most prognostic power in locally advanced or metastatic PC. Low FAR was positively correlated with OS in locally advanced or metastatic PC, which could be used to predict the prognosis.
全身性炎症反应是促进包括胰腺癌(PC)在内的恶性肿瘤发生和转移的关键因素。本研究旨在确定并比较中性粒细胞与淋巴细胞比值(NLR)、血小板与淋巴细胞比值(PLR)、单核细胞与淋巴细胞比值(MLR)和纤维蛋白原与白蛋白比值(FAR)在可切除 PC 与局部晚期或转移性 PC 中的预后价值。
本研究共纳入 353 例可切除 PC 患者和 807 例局部晚期或转移性 PC 患者。这些患者被分为训练集(n=758)和验证集(n=402)。采用 Kaplan-Meier 生存曲线和 Cox 比例风险回归模型分析预后。
术前 PLR(p=0.048)和 MLR(p=0.027)较低的可切除 PC 患者的总生存期(OS)明显更好。低 FAR、MLR、NLR(p<0.001)和 PLR(p=0.003)与局部晚期或转移性 PC 患者死亡风险降低显著相关。FAR(风险比[HR],1.522;95%置信区间[CI],1.261 至 1.837;p<0.001)和 MLR(HR,1.248;95%CI,1.017 至 1.532;p=0.034)是局部晚期或转移性 PC 的独立预后因素。
FAR、MLR、NLR 和 PLR 在可切除 PC 和局部晚期或转移性 PC 中的预后作用不同。FAR 在局部晚期或转移性 PC 中具有最强的预后能力。低 FAR 与局部晚期或转移性 PC 的 OS 呈正相关,可用于预测预后。