Department of Neurology, University of Erlangen-Nuremberg, Schwabachanlage 6, 91054, Erlangen, Germany.
Department of Neuroradiology, University of Erlangen-Nuremberg, Schwabachanlage 6, 91054, Erlangen, Germany.
Neurocrit Care. 2021 Aug;35(1):210-220. doi: 10.1007/s12028-020-01146-4. Epub 2020 Dec 24.
Although automated pupillometry is increasingly used in critical care settings, predictive value of automatically assessed pupillary parameters during different intracranial pressure (ICP) levels and possible clinical implications are unestablished.
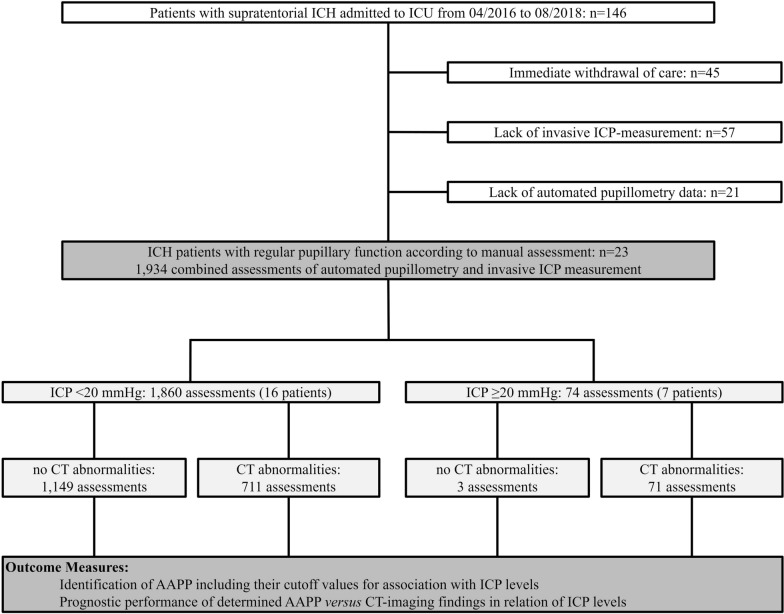
This retrospective cohort study at the neurocritical care unit of the University of Erlangen-Nuremberg (2016-2018) included 23 nontraumatic supratentorial (intracerebral hemorrhage) ICH patients without signs of abnormal pupillary function by manual assessment, i.e., absent light reflex. We assessed ICP levels by an external ventricular drain simultaneously with parameters of pupillary reactivity [i.e., maximum and minimum apertures, light reflex latency (Lat), constriction and redilation velocities (CV, DV), and percentage change of apertures (per-change)] using a portable pupillometer (NeurOptics®). Computed tomography (CT) scans were analyzed to determine lesion location, size, intraventricular hemorrhage, hydrocephalus, midline shift, and compression or absence of the basal cisterns. We performed receiver operating characteristics analysis to investigate associations of ICP levels with pupillary parameters and to determine best cutoff values for prediction of ICP elevation. After dichotomization of assessments according to ICP values (normal: < 20 mmHg, elevated: ≥ 20 mmHg), prognostic performance of the determined cutoff parameters of pupillary function versus of CT-imaging findings was analyzed by calculating sensitivity, specificity, positive and negative predictive values (logistic regression, corresponding ORs with 95% CIs).
In 23 patients (11 women, median age 59.0 (51.0-69.0) years), 1,934 assessments were available for analysis. A total of 74 ICP elevations ≥ 20 mmHg occurred in seven patients. Best discriminative thresholds for ICP elevation were: CV < 0.8 mm/s (AUC 0.740), per-change < 10% (AUC 0.743), DV < 0.2 mm/s (AUC 0.703), and Lat > 0.3 s (AUC 0.616). Positive predictive value of all four parameters to indicate ICP elevation ranged between 7.2 and 8.3% only and was similarly low for CT abnormalities (9.1%). We found high negative predictive values of pupillary parameters [CV: 99.2% (95% CI 98.3-99.6), per-change: 98.7% (95% CI 97.8-99.2), DV: 98.0% (95% CI 97.0-98.7), Lat: 97.0% (95% CI 96.0-97.7)], and CT abnormalities [99.7% (95% CI 99.2-99.9)], providing evidence that both techniques adequately identified ICH patients without ICP elevation.
Our data suggest an association between noninvasively detected changes in pupillary reactivity and ICP levels in sedated ICH patients. Although automated pupillometry and neuroimaging seem not sufficient to noninvasively indicate ICP elevation, both techniques, however, adequately identified ICH patients without ICP elevation. This finding may facilitate routine management by saving invasive ICP monitoring or repeated CT controls in patients with specific automated pupillometry readings.
尽管自动化瞳孔测量在重症监护环境中越来越多地被使用,但是在不同颅内压(ICP)水平下自动评估瞳孔参数的预测价值以及可能的临床意义尚未确定。
本研究是在纽伦堡大学神经重症监护病房进行的回顾性队列研究(2016-2018 年),纳入了 23 例非创伤性幕上(脑内出血)ICH 患者,这些患者通过手动评估(即光反射消失)没有异常瞳孔功能的迹象。我们通过外部脑室引流同时评估 ICP 水平,同时使用便携式瞳孔计(NeurOptics®)评估瞳孔反应参数[即最大和最小孔径、光反射潜伏期(Lat)、收缩和扩张速度(CV、DV)以及孔径变化百分比(per-change)]。进行计算机断层扫描(CT)扫描以确定病变位置、大小、脑室内出血、脑积水、中线移位以及基底池受压或缺失。我们进行了受试者工作特征(ROC)分析,以研究 ICP 水平与瞳孔参数的关联,并确定预测 ICP 升高的最佳截断值。根据 ICP 值(正常:<20mmHg,升高:≥20mmHg)对评估进行二分类后,通过计算敏感性、特异性、阳性和阴性预测值(逻辑回归,相应的 95%置信区间的比值比(OR)),分析确定的瞳孔功能与 CT 成像结果的预后性能。
在 23 例患者(11 名女性,中位年龄 59.0(51.0-69.0)岁)中,共有 1934 次评估可用于分析。7 名患者共发生 74 次 ICP 升高≥20mmHg。提示 ICP 升高的最佳判别阈值为:CV<0.8mm/s(AUC 0.740)、per-change<10%(AUC 0.743)、DV<0.2mm/s(AUC 0.703)和 Lat>0.3s(AUC 0.616)。四项参数中,所有参数预测 ICP 升高的阳性预测值均仅为 7.2%-8.3%,而 CT 异常的阳性预测值也相似(9.1%)。我们发现瞳孔参数的高阴性预测值[CV:99.2%(95%置信区间 98.3-99.6)、per-change:98.7%(95%置信区间 97.8-99.2)、DV:98.0%(95%置信区间 97.0-98.7)、Lat:97.0%(95%置信区间 96.0-97.7)]和 CT 异常[99.7%(95%置信区间 99.2-99.9)],这表明两种技术都能充分识别 ICH 患者中没有 ICP 升高的患者。
我们的数据表明,在镇静的 ICH 患者中,瞳孔反应的非侵入性检测变化与 ICP 水平之间存在关联。尽管自动瞳孔测量和神经影像学似乎不足以非侵入性地指示 ICP 升高,但这两种技术都能充分识别 ICH 患者中没有 ICP 升高的患者。这一发现可能通过在具有特定自动瞳孔测量读数的患者中节省有创 ICP 监测或重复 CT 检查来促进常规管理。