Department of Otolaryngology/Head and Neck Surgery, University of North Carolina at Chapel Hill, North Carolina, USA.
Department of Otolaryngology-Head and Neck Surgery, Washington University School of Medicine, St. Louis, Missouri, USA.
Ear Hear. 2021 July/Aug;42(4):941-948. doi: 10.1097/AUD.0000000000000985.
Electrocochleography (ECochG), obtained before the insertion of a cochlear implant (CI) array, provides a measure of residual cochlear function that accounts for a substantial portion of variability in postoperative speech perception outcomes in adults. It is postulated that subsequent surgical factors represent independent sources of variance in outcomes. Prior work has demonstrated a positive correlation between angular insertion depth (AID) of straight arrays and speech perception under the CI-alone condition, with an inverse relationship observed for precurved arrays. The purpose of the present study was to determine the combined effects of ECochG, AID, and array design on speech perception outcomes.
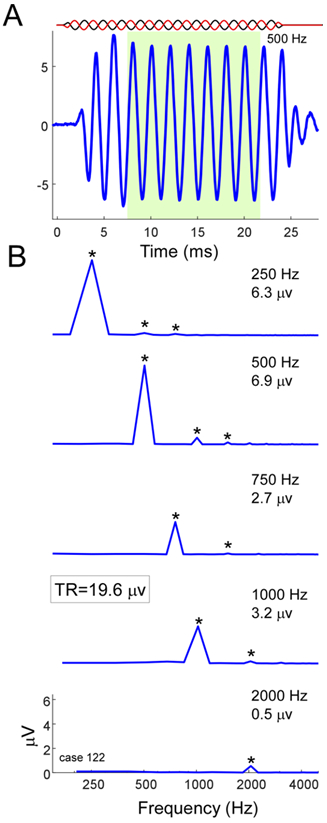
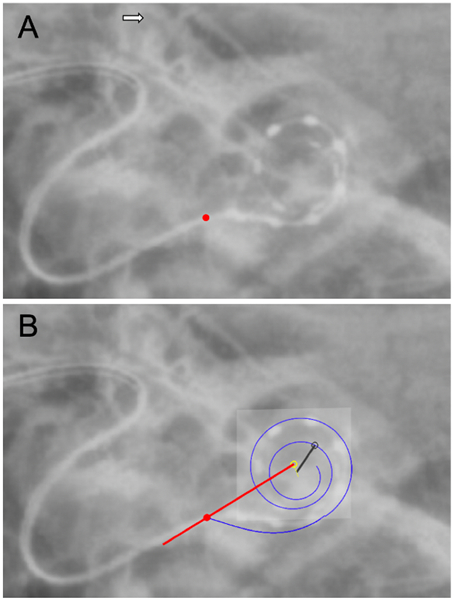
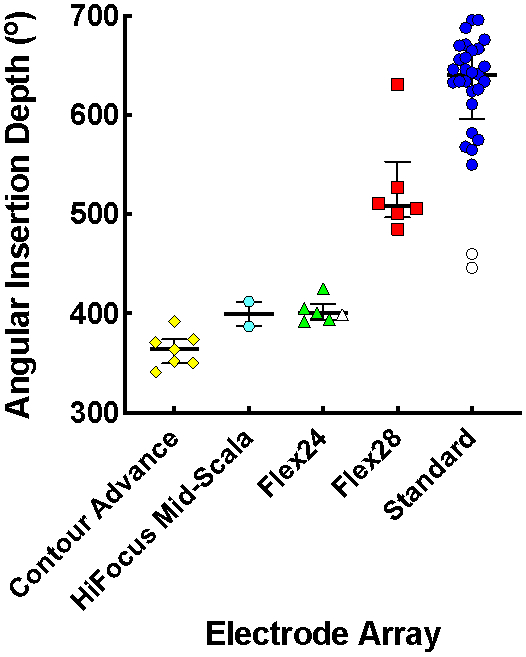
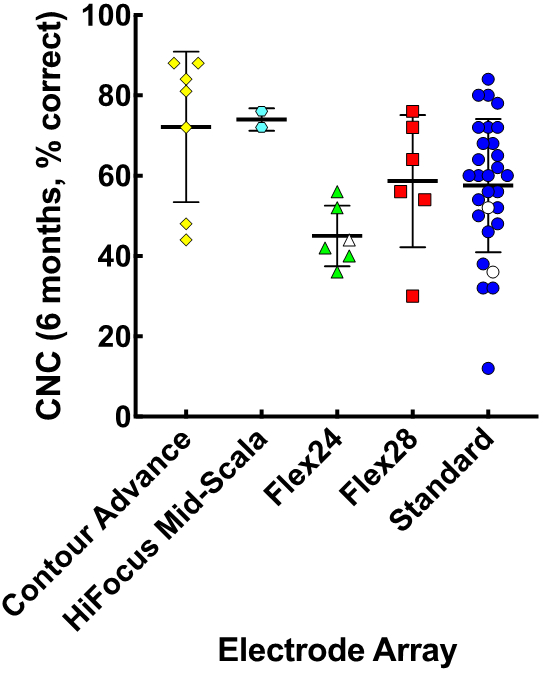
Participants were 50 postlingually deafened adult CI recipients who received one of three straight arrays (MED-EL Flex24, MED-EL Flex28, and MED-EL Standard) and two precurved arrays (Cochlear Contour Advance and Advanced Bionics HiFocus Mid-Scala). Residual cochlear function was determined by the intraoperative ECochG total response (TR) measured before array insertion, which is the sum of magnitudes of spectral components in response to tones of different stimulus frequencies across the speech spectrum. The AID was then determined with postoperative imaging. Multiple linear regression was used to predict consonant-nucleus-consonant (CNC) word recognition in the CI-alone condition at 6 months postactivation based on AID, TR, and array design.
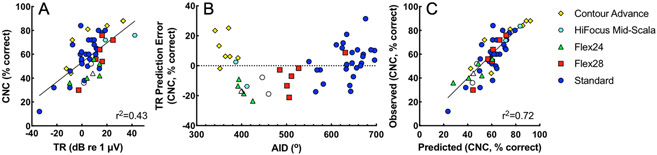
Forty-one participants received a straight array and nine received a precurved array. The AID of the most apical electrode contact ranged from 341° to 696°. The TR measured by ECochG accounted for 43% of variance in speech perception outcomes (p < 0.001). A regression model predicting CNC word scores with the TR tended to underestimate the performance for precurved arrays and deeply inserted straight arrays, and to overestimate the performance for straight arrays with shallower insertions. When combined in a multivariate linear regression, the TR, AID, and array design accounted for 72% of variability in speech perception outcomes (p < 0.001).
A model of speech perception outcomes that incorporates TR, AID, and array design represents an improvement over a model based on TR alone. The success of this model shows that peripheral factors including cochlear health and electrode placement may play a predominant role in speech perception with CIs.
在插入人工耳蜗(CI)数组之前获得的电 Cochleography(ECochG)提供了残余耳蜗功能的测量,该测量解释了成年人术后言语感知结果的很大一部分变异性。据推测,随后的手术因素是结果的独立方差源。先前的工作表明,直数组的角度插入深度(AID)与 CI 单独条件下的言语感知之间呈正相关,而对于预弯曲数组则观察到相反的关系。本研究的目的是确定 ECochG、AID 和数组设计对言语感知结果的综合影响。
参与者为 50 名后天失聪的成年 CI 接受者,他们接受了三种直数组(MED-EL Flex24、MED-EL Flex28 和 MED-EL Standard)和两种预弯曲数组(Cochlear Contour Advance 和 Advanced Bionics HiFocus Mid-Scala)之一。通过在插入数组之前测量的术中 ECochG 总反应(TR)来确定残余耳蜗功能,该值是响应不同刺激频率的音调的频谱分量幅度之和。然后通过术后成像确定 AID。使用多元线性回归根据 AID、TR 和数组设计预测 6 个月激活后 CI 单独条件下的辅音-核-辅音(CNC)单词识别。
41 名参与者接受了直数组,9 名参与者接受了预弯曲数组。最顶端电极接触的 AID 范围从 341°到 696°。ECochG 测量的 TR 占言语感知结果变异性的 43%(p < 0.001)。使用 TR 预测 CNC 单词得分的回归模型倾向于低估预弯曲数组和深度插入直数组的性能,高估浅插入直数组的性能。当结合多元线性回归时,TR、AID 和数组设计占言语感知结果变异性的 72%(p < 0.001)。
包含 TR、AID 和数组设计的言语感知结果模型比基于 TR 单独的模型有所改进。该模型的成功表明,包括耳蜗健康和电极放置在内的外围因素可能在 CI 中的言语感知中起主要作用。