Division of Pulmonary and Critical Care Medicine, Penn State Health Milton S Hershey Medical Center, Hershey, Pennsylvania, United States of America.
Department of Public Health Sciences, Penn State Health Milton S Hershey Medical Center, Hershey, Pennsylvania, United States of America.
PLoS One. 2020 Dec 28;15(12):e0243449. doi: 10.1371/journal.pone.0243449. eCollection 2020.
The incidence of sepsis has been rising overall but updated data in cancer patients are lacking. After a cancer diagnosis, incidence of sepsis and overall mortality peak within the first year. However, how much sepsis contributes to mortality remains unclear. We used a multistate model approach to analyze the incidence, risk factors and associated mortality of sepsis within 1 year of cancer diagnosis in middle aged adults.
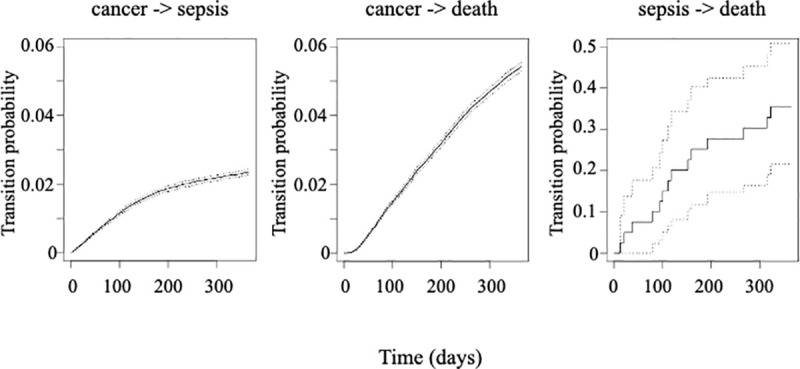
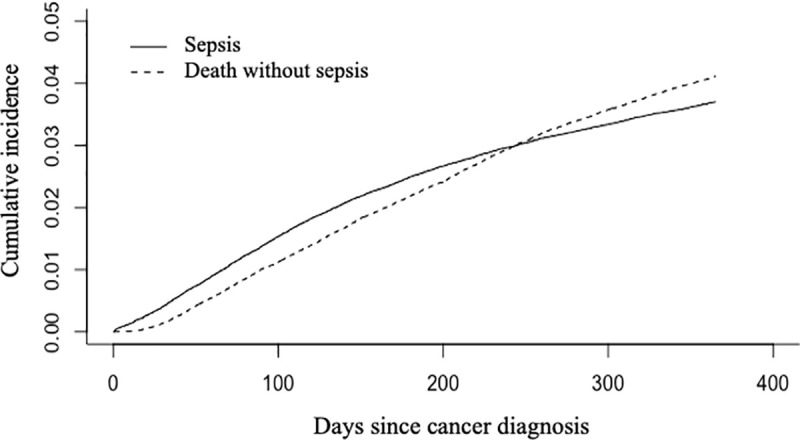
Analysis of a large US health insurance claims database (Marketscan) between 2005 and 2014. Patients with a new diagnosis of cancer who received chemotherapy were included. Within a year of diagnosis, we assessed inpatient admissions for sepsis based on ICD-9 codes and survival using hospitalizations, outpatient visits and prescriptions filled. Competing risk and multistate models were used to assess the incidence of sepsis and transition probabilities between cancer, sepsis and death.
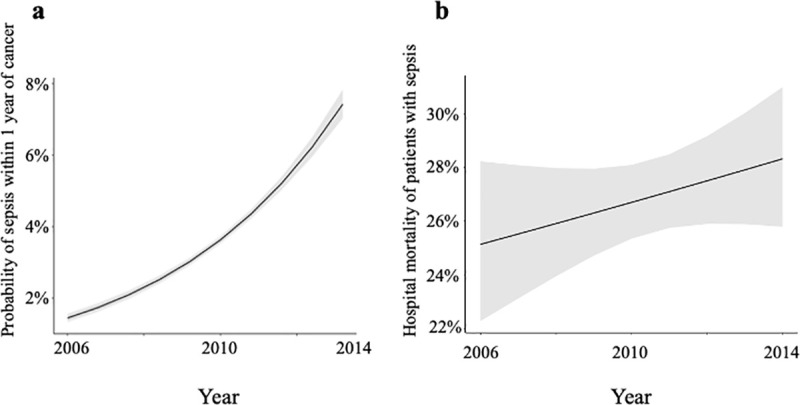
119,379 patients (38.9% males), aged 55 (50-60) years, were included; 2,560 developed isolated sepsis, 477 severe sepsis and 1331 septic shock within 1 year, with associated hospital mortality of 14.8%, 30% and 46% respectively. The probability of sepsis increased between 2005 and 2014; at 1 year, its cumulative incidence was 3.7% with a probability of mortality after sepsis of 35.5% (95% CI 21.6%-50.9%). Age, male gender, Charlson comorbidity index, hematological malignancies and metastases at diagnosis were associated with sepsis and mortality.
Incidence and mortality of sepsis were 3.7% and 35.5% at 1 year after cancer diagnosis and were both associated with baseline patient and cancer characteristics.
脓毒症的发病率总体呈上升趋势,但癌症患者的最新数据仍有所欠缺。癌症确诊后,脓毒症的发病率和总死亡率在最初一年内达到峰值。然而,脓毒症对死亡率的影响程度仍不清楚。我们采用多状态模型方法分析了中年癌症患者确诊后 1 年内脓毒症的发病率、危险因素及相关死亡率。
分析了 2005 年至 2014 年间美国大型医疗保险索赔数据库(Marketscan)的数据。纳入了新诊断为癌症且接受化疗的患者。在确诊后 1 年内,我们根据 ICD-9 编码评估了脓毒症的住院情况,并通过住院、门诊就诊和处方用药评估了生存情况。采用竞争风险和多状态模型评估了脓毒症的发病率以及癌症、脓毒症和死亡之间的转移概率。
共纳入 119379 名(38.9%为男性)年龄为 55(50-60)岁的患者;其中 2560 例患者确诊为单纯性脓毒症,477 例患者为严重脓毒症,1331 例患者为脓毒性休克,住院死亡率分别为 14.8%、30%和 46%。2005 年至 2014 年间,脓毒症的发病率呈上升趋势;1 年后,其累积发病率为 3.7%,脓毒症后死亡率为 35.5%(95%CI 21.6%-50.9%)。年龄、男性、Charlson 合并症指数、血液系统恶性肿瘤和诊断时转移与脓毒症和死亡率相关。
癌症确诊后 1 年,脓毒症的发病率和死亡率分别为 3.7%和 35.5%,且均与患者基线特征和癌症特征相关。