Comisión Asesora de Programa de Salud Renal, Fondo Nacional de Recursos, Montevideo, Uruguay.
Departamento de Nefrología, Facultad de Medicina, Universidad de la República, Montevideo, Uruguay.
PLoS One. 2022 Oct 14;17(10):e0266617. doi: 10.1371/journal.pone.0266617. eCollection 2022.
The Renal Healthcare Program Uruguay (NRHP-UY) is a national, multidisciplinary program that provides care to chronic kidney disease (CKD) patients. In this study, we report the global results of CKD patient outcomes and a comparison between those treated at the NRHP-UY Units, with those patients who were initially included in the program but did not adhere to follow up.
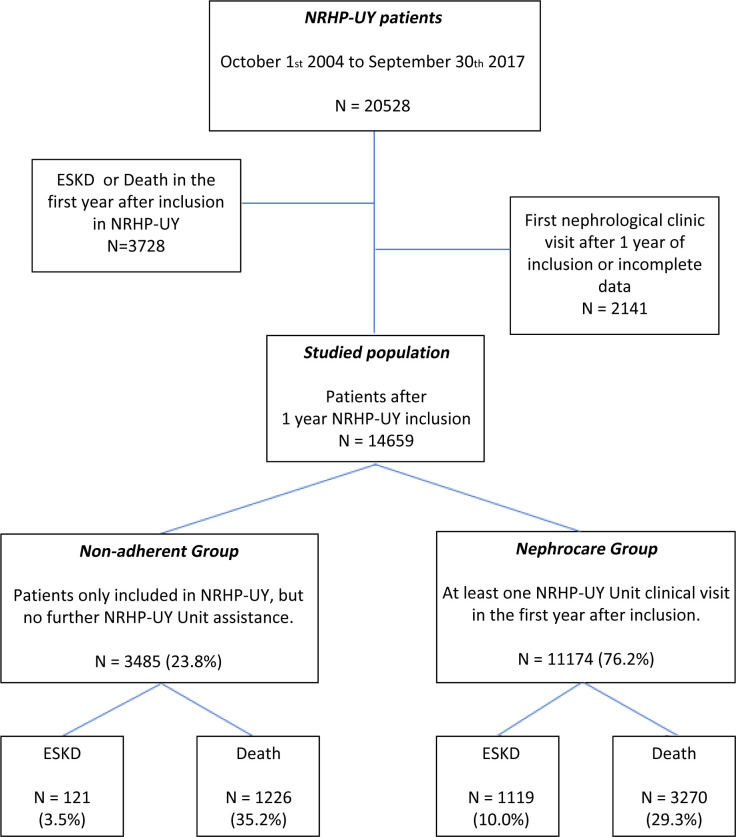
A cohort of not-on dialysis CKD patients included prospectively in the NRHP-UY between October 1st 2004 and September 30th 2017 was followed-up until September 30th 2019. Two groups were compared: a) Nephrocare Group: Patients who had at least one clinic visit during the first year on NRHP-UY (n = 11174) and b) Non-adherent Group: Patients who were informed and accepted to be included but had no subsequent data registered after admission (n = 3485). The study was approved by the Ethics Committee and all patients signed an informed consent. Outcomes were studied with Logistic and Cox´s regression analysis, Fine and Gray competitive risk and propensity-score matching tests.
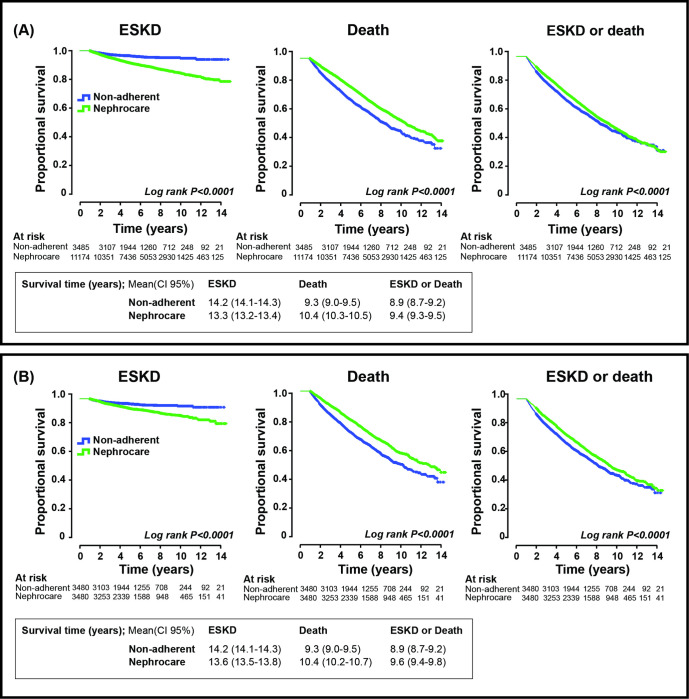
14659 patients were analyzed, median age 70 (60-77) years, 56.9% male. The Nephrocare Group showed improved achievement of therapeutic goals, ESKD was more frequent (HR 2.081, CI 95%1.722-2.514) as planned kidney replacement therapy (KRT) start (OR 2.494, CI95% 1.591-3.910), but mortality and the combined event (death and ESKD) were less frequent (HR 0.671, CI95% 0.628-0.717 and 0.777, CI95% 0.731-0.827) (p = 0.000) compared to the Non-adherent group. Results were similar in the propensity-matched group: ESKD (HR 2.041, CI95% 1.643-2.534); planned kidney replacement therapy (KRT) start (OR 2.191, CI95% 1.322-3.631) death (HR 0.692, CI95% 0.637-0.753); combined event (HR 0.801, CI95% 0.742-0.865) (p = 0.000).
Multidisciplinary care within the NRHP-UY is associated with timely initiation of KRT and lower mortality in single outcomes, combined analysis, and propensity-matched analysis.
乌拉圭肾脏保健计划(NRHP-UY)是一个全国性的多学科项目,为慢性肾脏病(CKD)患者提供护理。在这项研究中,我们报告了 CKD 患者结局的全球结果,并比较了在 NRHP-UY 单位接受治疗的患者与最初纳入该计划但未坚持随访的患者。
2004 年 10 月 1 日至 2017 年 9 月 30 日期间,前瞻性纳入 NRHP-UY 的非透析 CKD 患者队列进行随访,直至 2019 年 9 月 30 日。比较了两组:a)肾保健组:至少有一次在 NRHP-UY 第一年就诊的患者(n=11174)和 b)不依从组:已告知并接受纳入但入院后无后续数据登记的患者(n=3485)。该研究得到了伦理委员会的批准,所有患者均签署了知情同意书。使用 Logistic 和 Cox 回归分析、Fine 和 Gray 竞争风险和倾向评分匹配检验研究了结局。
分析了 14659 名患者,中位年龄为 70(60-77)岁,56.9%为男性。肾保健组实现治疗目标的情况有所改善,计划肾脏替代治疗(KRT)开始时更频繁地发生终末期肾病(ESKD)(HR 2.081,95%CI 1.722-2.514)(OR 2.494,95%CI 1.591-3.910),但死亡率和复合事件(死亡和 ESKD)的发生率较低(HR 0.671,95%CI 0.628-0.717 和 0.777,95%CI 0.731-0.827)(p=0.000)与不依从组相比。在倾向评分匹配组中,结果相似:ESKD(HR 2.041,95%CI 1.643-2.534);计划肾脏替代治疗(KRT)开始(OR 2.191,95%CI 1.322-3.631)死亡(HR 0.692,95%CI 1.637-0.753);复合事件(HR 0.801,95%CI 1.742-0.865)(p=0.000)。
NRHP-UY 内的多学科护理与及时启动 KRT 相关,并降低单结局、综合分析和倾向评分匹配分析中的死亡率。