Department of Orthopaedic Surgery, Anam Hospital, Korea University College of Medicine, Seoul 02841, Korea.
Department of Sports Medical Center, Anam Hospital, Korea University College of Medicine, Seoul 02841, Korea.
Medicina (Kaunas). 2020 Dec 28;57(1):19. doi: 10.3390/medicina57010019.
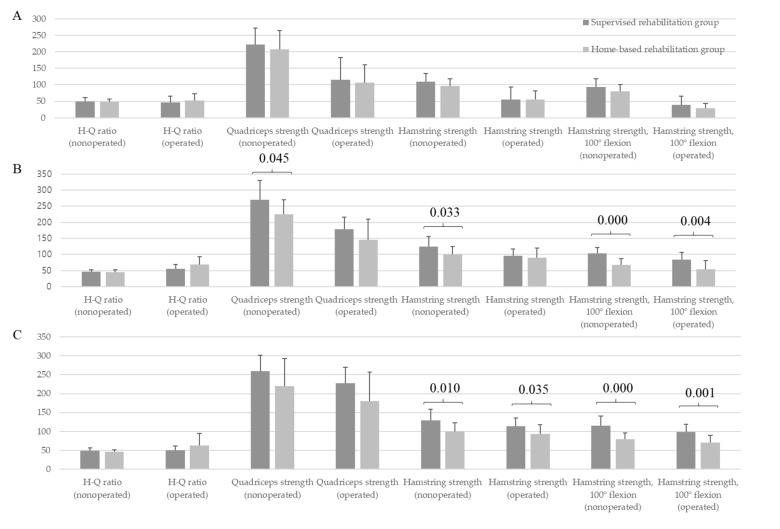
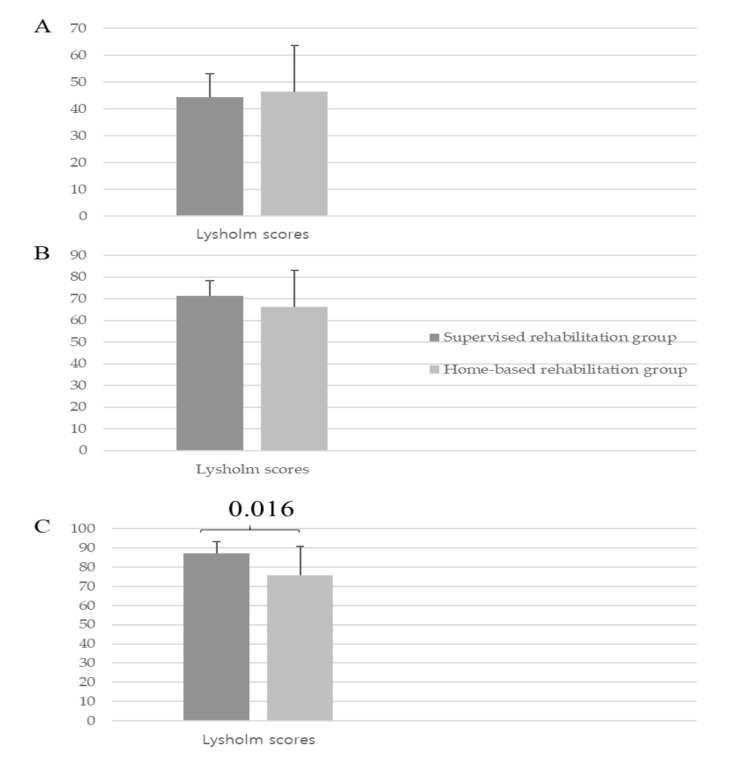
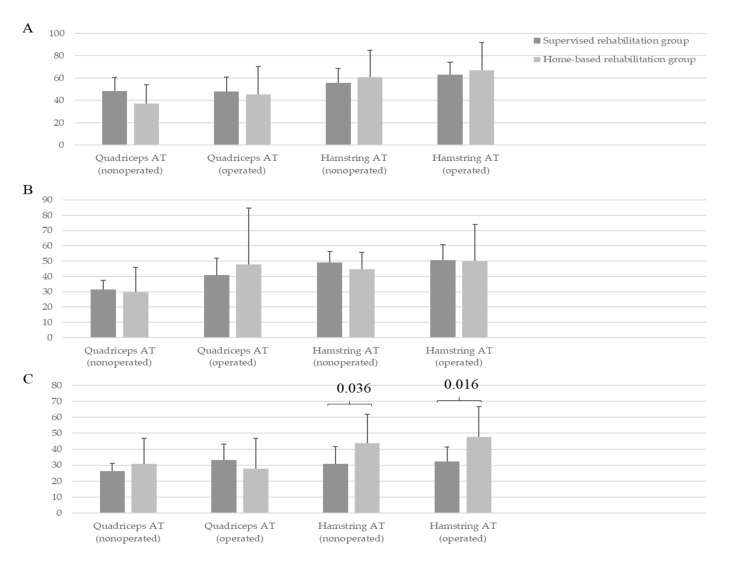
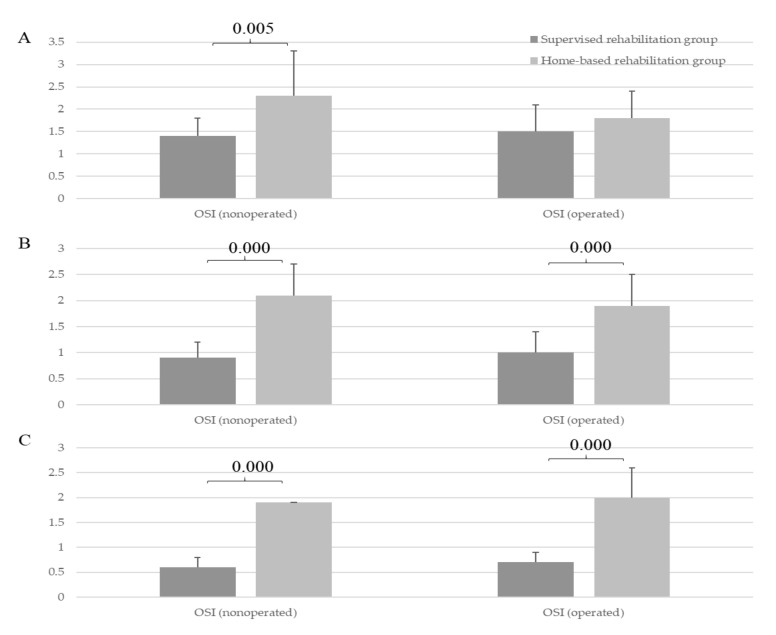
Previous studies consistently found no significant difference between supervised and home-based rehabilitation after anterior cruciate ligament reconstruction (ACLR). However, the function of the nonoperative knee, hamstring strength at deep flexion, and neuromuscular control have been overlooked. This prospective observational study was performed to investigate the outcomes after ACLR in operative and nonoperative knees between supervised and home-based rehabilitations. After surgery, instructional videos demonstrating the rehabilitation process and exercises were provided for the home-based rehabilitation group. The supervised rehabilitation group visited our sports medicine center and physical therapists followed up all patients during the entire duration of the study. Isokinetic muscle strength and neuromuscular control (acceleration time (AT) and overall stability index (OSI)) of both operative and nonoperative knees, as well as patient-reported knee function (Lysholm score), were measured and compared between the two groups 6 months and 1 year postoperatively. The supervised rehabilitation group showed higher muscle strength of hamstring and quadriceps in nonoperative knees at 6 months (hamstring, = 0.033; quadriceps, = 0.045) and higher hamstring strength in operative and nonoperative knees at 1 year (operative knees, = 0.035; nonoperative knees, = 0.010) than the home-based rehabilitation group. At 6 months and 1 year, OSIs in operative and nonoperative knees were significantly better in the supervised rehabilitation group than in the home-based rehabilitation group (operative knees, < 0.001, < 0.001; nonoperative knees, < 0.001, < 0.001, at 6 months and 1 year, respectively). At 1 year, the supervised rehabilitation group also demonstrated faster AT of the hamstrings (operative knees, = 0.016; nonoperative knees, = 0.036). Lysholm scores gradually improved in both groups over 1 year; however, the supervised rehabilitation group showed higher scores at 1 year (87.3 ± 5.8 vs. 75.6 ± 15.1, = 0.016). This study demonstrated that supervised rehabilitation may offer additional benefits in improving muscle strength, neuromuscular control, and patient-reported knee function compared with home-based rehabilitation up to 1 year after ACLR.
先前的研究一致表明,在前交叉韧带重建(ACLR)后,监督式康复和家庭康复之间没有显著差异。然而,非手术膝关节的功能、屈膝时腘绳肌的力量和神经肌肉控制已经被忽视了。这项前瞻性观察研究旨在调查 ACLR 后手术和非手术膝关节在监督式康复和家庭康复之间的结果。手术后,为家庭康复组提供了演示康复过程和练习的教学视频。监督式康复组访问了我们的运动医学中心,物理治疗师在整个研究期间对所有患者进行了随访。在手术后 6 个月和 1 年,测量并比较了两组患者手术和非手术膝关节的等速肌肉力量和神经肌肉控制(加速时间(AT)和整体稳定性指数(OSI))以及患者报告的膝关节功能(Lysholm 评分)。监督式康复组在术后 6 个月时非手术膝关节的腘绳肌和股四头肌力量较高(腘绳肌,=0.033;股四头肌,=0.045),在术后 1 年时手术和非手术膝关节的腘绳肌力量较高(手术膝关节,=0.035;非手术膝关节,=0.010)。在术后 6 个月和 1 年,手术和非手术膝关节的 OSI 在监督式康复组明显优于家庭康复组(手术膝关节,<0.001,<0.001;非手术膝关节,<0.001,<0.001,分别在术后 6 个月和 1 年)。在术后 1 年,监督式康复组还表现出更快的腘绳肌 AT(手术膝关节,=0.016;非手术膝关节,=0.036)。Lysholm 评分在 1 年内逐渐提高,但监督式康复组在 1 年时得分较高(87.3±5.8 与 75.6±15.1,=0.016)。这项研究表明,与家庭康复相比,监督式康复在 ACLR 后 1 年内可能提供额外的益处,可改善肌肉力量、神经肌肉控制和患者报告的膝关节功能。