Department of Anesthesiology, Affiliated Hospital of Guangdong Medical University, Zhanjiang, China.
Department of Anaesthesiology, The University of Hong Kong, Hong Kong, SAR, China.
Cardiovasc Diabetol. 2021 Jan 4;20(1):2. doi: 10.1186/s12933-020-01188-0.
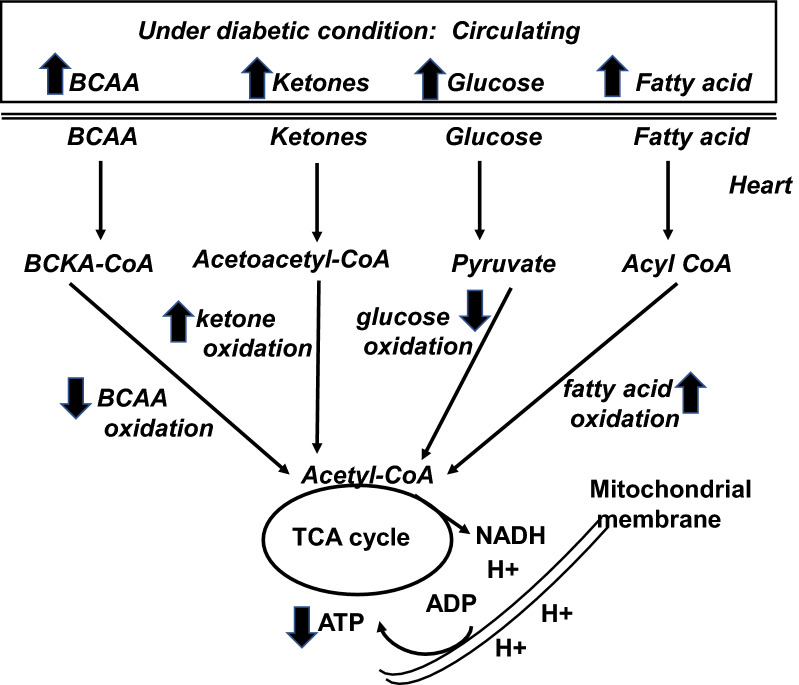
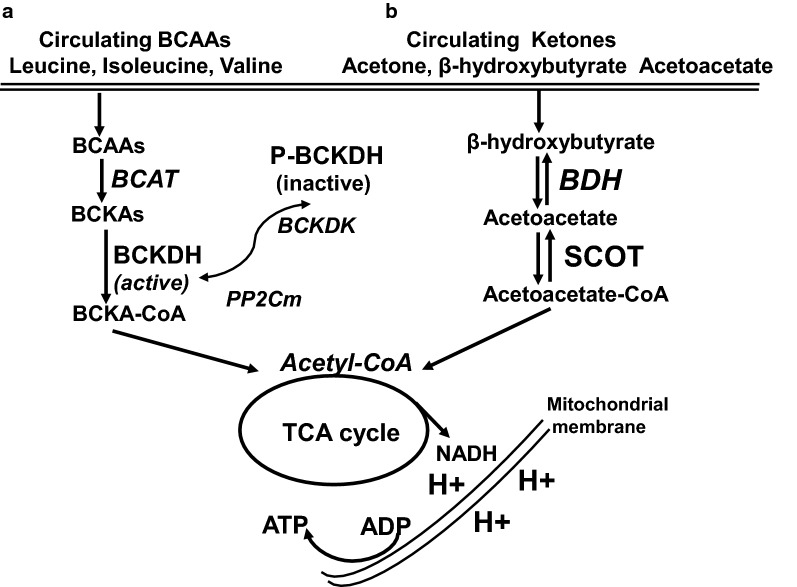
The prevalence of cardiomyopathy is higher in diabetic patients than those without diabetes. Diabetic cardiomyopathy (DCM) is defined as a clinical condition of abnormal myocardial structure and performance in diabetic patients without other cardiac risk factors, such as coronary artery disease, hypertension, and significant valvular disease. Multiple molecular events contribute to the development of DCM, which include the alterations in energy metabolism (fatty acid, glucose, ketone and branched chain amino acids) and the abnormalities of subcellular components in the heart, such as impaired insulin signaling, increased oxidative stress, calcium mishandling and inflammation. There are no specific drugs in treating DCM despite of decades of basic and clinical investigations. This is, in part, due to the lack of our understanding as to how heart failure initiates and develops, especially in diabetic patients without an underlying ischemic cause. Some of the traditional anti-diabetic or lipid-lowering agents aimed at shifting the balance of cardiac metabolism from utilizing fat to glucose have been shown inadequately targeting multiple aspects of the conditions. Peroxisome proliferator-activated receptor α (PPARα), a transcription factor, plays an important role in mediating DCM-related molecular events. Pharmacological targeting of PPARα activation has been demonstrated to be one of the important strategies for patients with diabetes, metabolic syndrome, and atherosclerotic cardiovascular diseases. The aim of this review is to provide a contemporary view of PPARα in association with the underlying pathophysiological changes in DCM. We discuss the PPARα-related drugs in clinical applications and facts related to the drugs that may be considered as risky (such as fenofibrate, bezafibrate, clofibrate) or safe (pemafibrate, metformin and glucagon-like peptide 1-receptor agonists) or having the potential (sodium-glucose co-transporter 2 inhibitor) in treating DCM.
扩张型心肌病在糖尿病患者中的发病率高于非糖尿病患者。糖尿病心肌病(DCM)定义为在无其他心脏危险因素(如冠状动脉疾病、高血压和显著瓣膜疾病)的糖尿病患者中出现异常心肌结构和功能的临床情况。多种分子事件导致 DCM 的发生,包括能量代谢(脂肪酸、葡萄糖、酮体和支链氨基酸)的改变以及心脏亚细胞成分的异常,如胰岛素信号转导受损、氧化应激增加、钙处理异常和炎症。尽管经过几十年的基础和临床研究,DCM 仍没有特定的治疗药物。这在一定程度上是由于我们对心力衰竭的发生和发展机制缺乏了解,尤其是在没有潜在缺血原因的糖尿病患者中。一些旨在将心脏代谢从利用脂肪转向葡萄糖的传统抗糖尿病或降脂药物,在针对这些疾病的多个方面时效果并不理想。过氧化物酶体增殖物激活受体α(PPARα)是一种转录因子,在介导 DCM 相关分子事件中发挥重要作用。已证明药物靶向激活 PPARα 是糖尿病、代谢综合征和动脉粥样硬化性心血管疾病患者的重要策略之一。本综述的目的是提供有关 PPARα 与 DCM 潜在病理生理变化的现代观点。我们讨论了临床应用中与 PPARα 相关的药物以及与可能有风险(如非诺贝特、苯扎贝特、氯贝特)或安全(培马贝特、二甲双胍和胰高血糖素样肽 1 受体激动剂)或有潜力(钠-葡萄糖共转运蛋白 2 抑制剂)的药物相关的事实。