Joint Department of Biomedical Engineering University of North Carolina and North Carolina State University NC.
Division of Cardiology University of North Carolina School of Medicine NC.
J Am Heart Assoc. 2021 Jan 19;10(2):e018414. doi: 10.1161/JAHA.120.018414. Epub 2021 Jan 5.
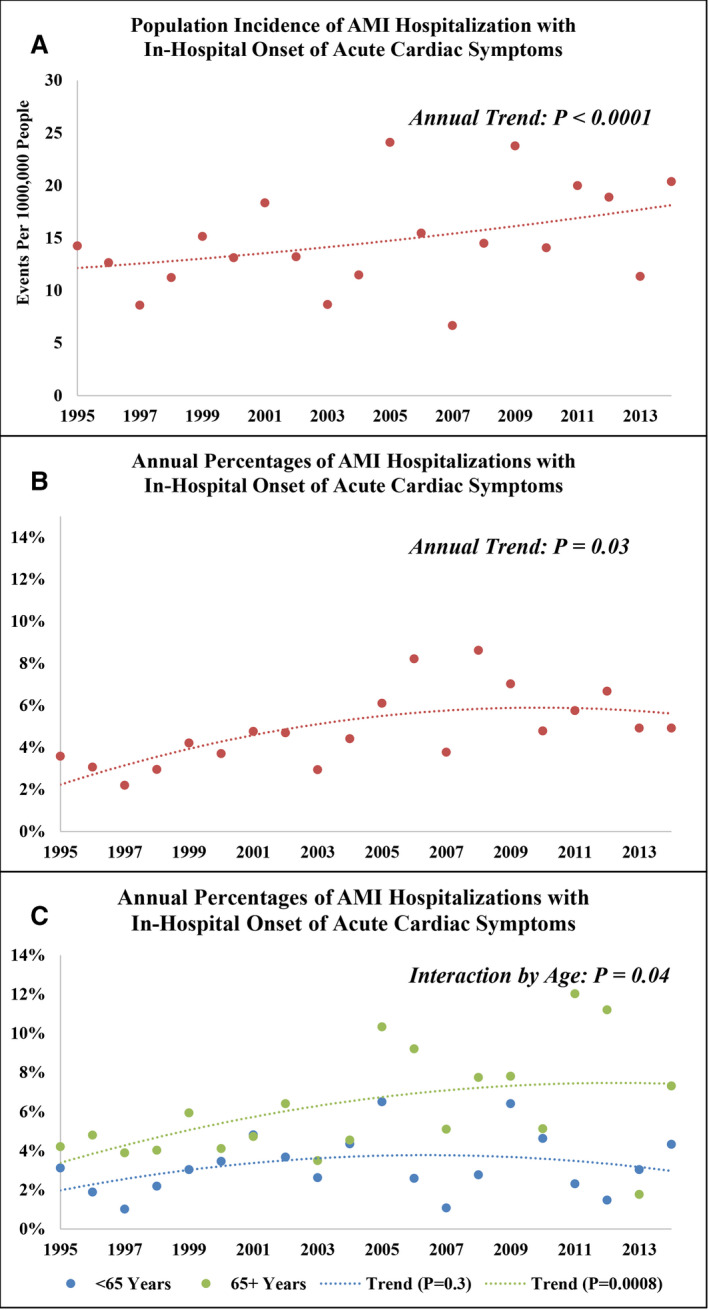
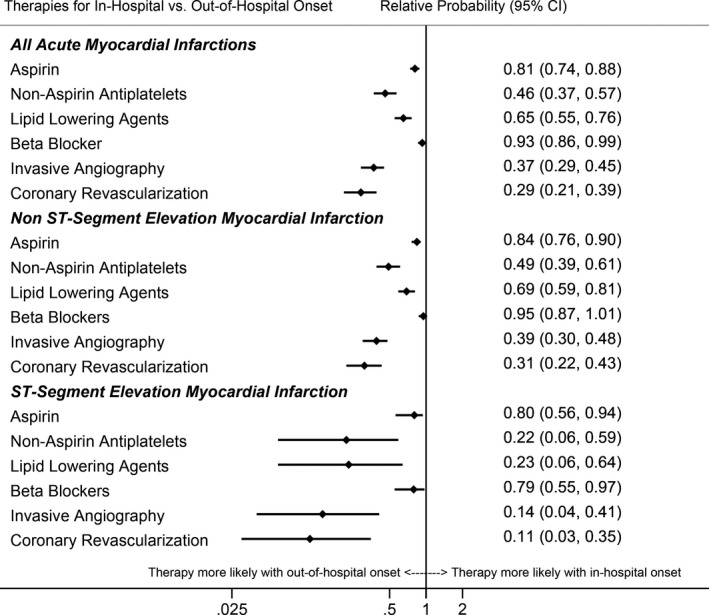
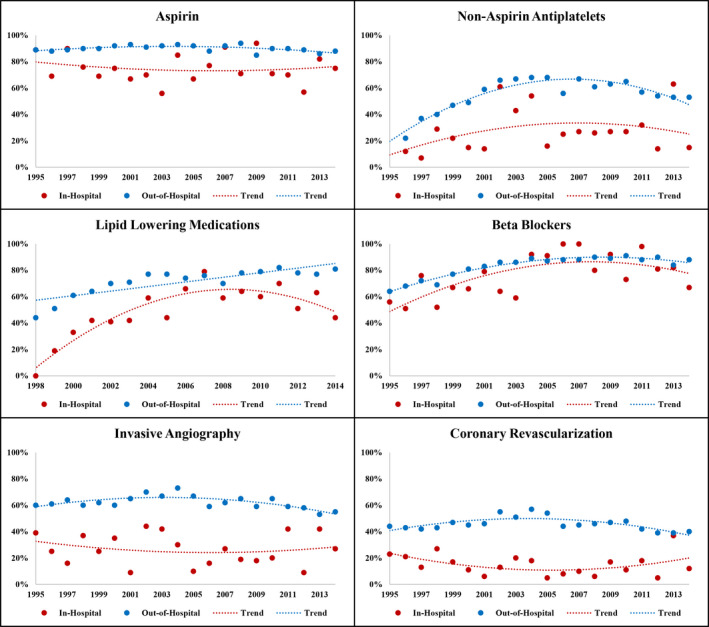
Background Acute myocardial infarction (AMI) with in-hospital onset (AMI-IHO) has poor prognosis but is clinically underappreciated. Whether its occurrence has changed over time is uncertain. Methods and Results Since 1987, the ARIC (Atherosclerosis Risk in Communities) study has conducted adjudicated surveillance of AMI hospitalizations in 4 US communities. Our analysis was limited to patients aged 35 to 74 years with symptomatic AMI. Patients with symptoms initiating after hospital arrival were considered AMI-IHO. A total of 26 678 weighted hospitalizations (14 276 unweighted hospitalizations) for symptomatic AMI were identified from 1995 to 2014, with 1137 (4%) classified as in-hospital onset. The population incidence rate of AMI-IHO increased in the 4 ARIC communities from 1995 through 2004 to 2005 through 2014 (12.7-16.9 events per 100 000 people; for 20-year trend <0.0001), as did the proportion of AMI hospitalizations with in-hospital onset (3.7%-6.1%; for 20-year trend =0.03). The 10-year proportions were stable for patients aged 35 to 64 years (3.0%-3.4%; for 20-year trend =0.3) but increased for patients aged ≥65 years (4.6%-7.8%; for 20-year trend =0.008; for interaction by age group =0.04). AMI-IHO had a more severe clinical course with lower use of AMI therapies or invasive strategies and higher in-hospital (7% versus 3%), 28-day (19% versus 5%), and 1-year (29% versus 12%) mortality (0.0001 for all). Conclusions In this population-based community surveillance, AMI-IHO increased from 2005 to 2014, particularly among older patients. Quality initiatives to improve recognition and management of AMI-IHO should be especially focused on hospitalized patients aged >65.
院内起病的急性心肌梗死(AMI-IHO)预后较差,但临床上未得到充分重视。其发生是否随时间而变化尚不确定。
自 1987 年以来,ARIC(社区动脉粥样硬化风险)研究对美国 4 个社区的 AMI 住院患者进行了裁定监测。我们的分析仅限于年龄在 35 至 74 岁、有症状性 AMI 的患者。症状在入院后开始的患者被认为是 AMI-IHO。从 1995 年到 2014 年,共确定了 26678 例有症状性 AMI 的加权住院病例(14276 例未加权住院病例),其中 1137 例(4%)为院内起病。ARIC 4 个社区的 AMI-IHO 人群发生率从 1995 年至 2004 年增加到 2005 年至 2014 年(每 10 万人 12.7-16.9 例;20 年趋势<0.0001),同时,院内起病的 AMI 住院患者比例也从 3.7%增加到 6.1%(20 年趋势=0.03)。对于年龄在 35 至 64 岁的患者,10 年的比例保持稳定(3.0%-3.4%;20 年趋势=0.3),但对于年龄≥65 岁的患者,该比例则有所增加(4.6%-7.8%;20 年趋势=0.008;按年龄组的交互作用=0.04)。AMI-IHO 的临床病程更严重,AMI 治疗或介入策略的应用率更低,住院(7%比 3%)、28 天(19%比 5%)和 1 年(29%比 12%)死亡率更高(所有 P<0.0001)。
在这项基于人群的社区监测中,AMI-IHO 从 2005 年至 2014 年有所增加,特别是在老年患者中。为了改善对 AMI-IHO 的识别和管理,应特别关注年龄大于 65 岁的住院患者。