Minneapolis Heart Institute, Minneapolis, Minnesota.
Minneapolis Heart Institute Foundation, Minneapolis, Minnesota.
JAMA Netw Open. 2019 Jan 4;2(1):e187348. doi: 10.1001/jamanetworkopen.2018.7348.
Studies of acute myocardial infarction (AMI) occurring outside the hospital have informed approaches to addressing risk, treatment, and patient outcomes. Similar insights for in-hospital AMI are lacking.
To determine the incidence, risk factors, and outcomes associated with in-hospital AMI.
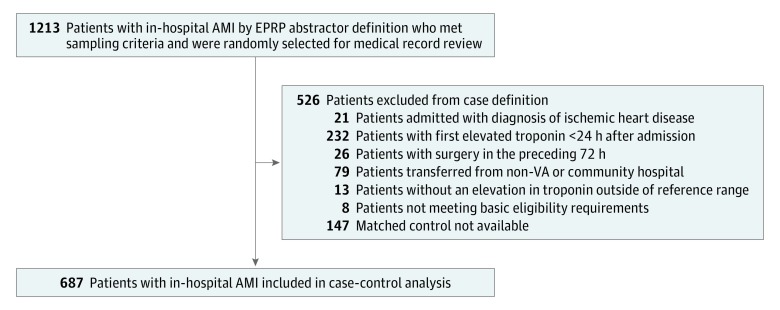
DESIGN, SETTING, AND PARTICIPANTS: Cohort, nested case-control, and matched cohort study of patients hospitalized in US Veterans Health Administration facilities between July 2007 and September 2009. The incidence of in-hospital AMI was determined from a complete cohort of in-hospital AMI relative to the total number of inpatient admissions. From the in-hospital AMI cohort, detailed medical record review was performed on 687 cases and 687 individually matched controls. Risk factors and outcomes associated with in-hospital AMI were determined from matched comparison of in-hospital AMI cases to hospitalized controls.
Candidate risk factors for in-hospital AMI included characteristics at the time of admission and in-hospital variables prior to the index date.
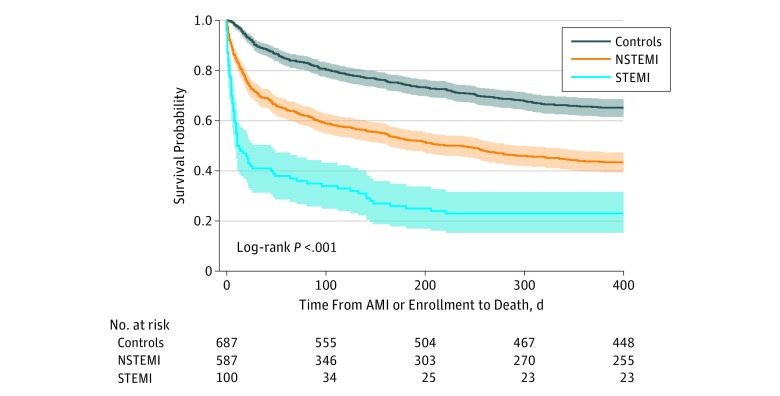
In the determination of the incidence and risk factors associated with in-hospital AMI, the outcome of interest was in-hospital AMI. All-cause mortality was the main outcome of interest following in-hospital AMI.
A total of 5556 patients with in-hospital AMI (mean [SD] age, 73 [10] years; 5456 [98.2%] male) were identified among 1.3 million admissions, with an incidence of 4.27 in-hospital AMI events per 1000 admissions. Independent risk factors associated with in-hospital AMI included intensive care unit setting, history of coronary artery disease, heart rate greater than 100 beats/min, hemoglobin level less than 8 g/dL, and white blood cell count 14 000/μL or greater. Compared with the matched control group, mortality was significantly higher for patients with in-hospital AMI (in-hospital mortality, 26.4% vs 4.2%; 30-day mortality, 33.0% vs 10.0%; 1-year mortality, 59.2% vs 34.4%).
In-hospital AMI was common and associated with common cardiovascular risk factors and markers of acute illness. Patient outcomes following in-hospital AMI were poor, with 1-year mortality approaching 60%. Further study of in-hospital AMI may yield opportunities to reduce in-hospital AMI risk and improve patient outcomes.
对院外发生的急性心肌梗死(AMI)的研究为评估风险、治疗和患者预后提供了依据。但对于院内 AMI 缺乏类似的深入了解。
确定院内 AMI 的发生率、危险因素和结局。
设计、地点和参与者:这是一项在美国退伍军人健康管理局(Veterans Health Administration)机构住院患者中进行的队列、巢式病例对照和匹配队列研究。通过院内 AMI 相对住院人数的完整队列来确定院内 AMI 的发生率。从院内 AMI 队列中,对 687 例病例和 687 例单独匹配的对照进行详细的病历回顾。通过匹配院内 AMI 病例与住院对照,确定与院内 AMI 相关的危险因素和结局。
与院内 AMI 相关的候选危险因素包括入院时的特征和索引日期前的院内变量。
在确定与院内 AMI 相关的发生率和危险因素时,感兴趣的结局是院内 AMI。院内 AMI 后的全因死亡率是主要观察结局。
在 130 万例住院患者中,共确定了 5556 例院内 AMI(平均[标准差]年龄为 73[10]岁;5456[98.2%]为男性),院内 AMI 的发生率为每 1000 例住院患者中有 4.27 例。与院内 AMI 相关的独立危险因素包括重症监护病房环境、冠状动脉疾病史、心率大于 100 次/分、血红蛋白水平小于 8g/dL 和白细胞计数大于等于 14000/μL。与匹配对照组相比,院内 AMI 患者的死亡率显著更高(院内死亡率 26.4%比 4.2%;30 天死亡率 33.0%比 10.0%;1 年死亡率 59.2%比 34.4%)。
院内 AMI 很常见,与常见的心血管危险因素和急性疾病标志物有关。院内 AMI 后的患者预后较差,1 年死亡率接近 60%。对院内 AMI 的进一步研究可能为降低院内 AMI 风险和改善患者预后提供机会。