Brkic Sime, Meyer Sara C
Department of Biomedicine, University Hospital Basel and University of Basel, Switzerland.
Division of Hematology, University Hospital Basel, Switzerland.
Hemasphere. 2020 Dec 29;5(1):e516. doi: 10.1097/HS9.0000000000000516. eCollection 2021 Jan.
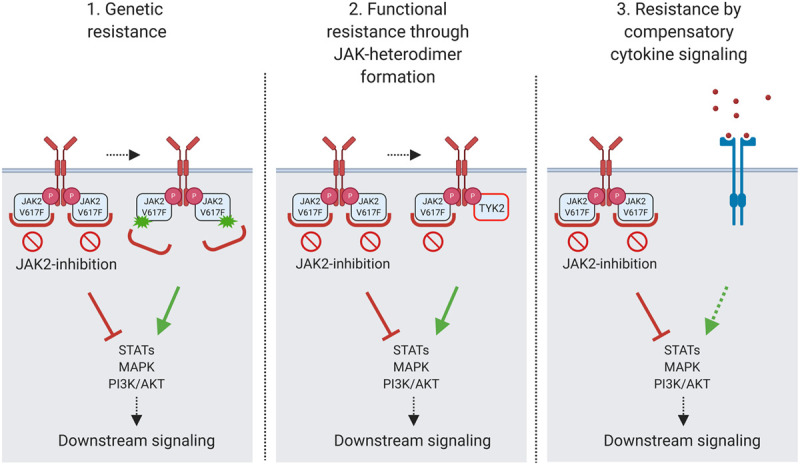
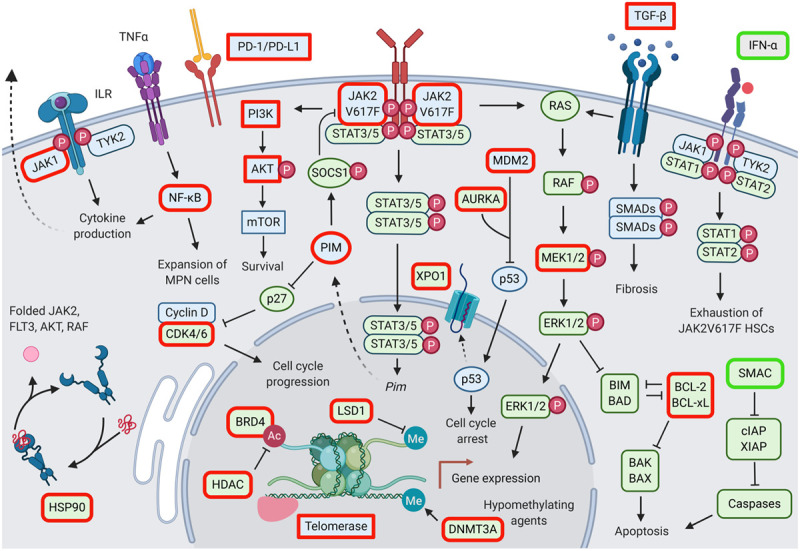
Myeloproliferative neoplasms (MPNs) are hematopoietic stem cell disorders with dysregulated myeloid blood cell production and propensity for transformation to acute myeloid leukemia, thrombosis, and bleeding. Acquired mutations in , , and converge on hyperactivation of Janus kinase 2 (JAK2) signaling as a central feature of MPN. Accordingly, JAK2 inhibitors have held promise for therapeutic targeting. After the JAK1/2 inhibitor ruxolitinib, similar JAK2 inhibitors as fedratinib are entering clinical use. While patients benefit with reduced splenomegaly and symptoms, disease-modifying effects on MPN clone size and clonal evolution are modest. Importantly, response to ruxolitinib may be lost upon treatment suggesting the MPN clone acquires resistance. Resistance mutations, as seen with other tyrosine kinase inhibitors, have not been described in MPN patients suggesting that functional processes reactivate JAK2 signaling. Compensatory signaling, which bypasses JAK2 inhibition, and other processes contribute to intrinsic resistance of MPN cells restricting efficacy of JAK2 inhibition overall. Combinations of JAK2 inhibition with pegylated interferon-α, a well-established therapy of MPN, B-cell lymphoma 2 inhibition, and others are in clinical development with the potential to enhance therapeutic efficacy. Novel single-agent approaches targeting other molecules than JAK2 are being investigated clinically. Special focus should be placed on myelofibrosis patients with anemia and thrombocytopenia, a delicate patient population at high need for options. The extending range of new treatment approaches will increase the therapeutic options for MPN patients. This calls for concomitant improvement of our insight into MPN biology to inform tailored therapeutic strategies for individual MPN patients.
骨髓增殖性肿瘤(MPN)是造血干细胞疾病,其髓系血细胞生成失调,易于转化为急性髓系白血病、血栓形成和出血。JAK2、MPL和CALR基因的获得性突变均导致Janus激酶2(JAK2)信号通路过度激活,这是MPN的核心特征。因此,JAK2抑制剂具有治疗靶点的前景。继JAK1/2抑制剂鲁索替尼之后,类似的JAK2抑制剂如非达替尼也进入了临床应用。虽然患者的脾肿大和症状有所减轻,但对MPN克隆大小和克隆进化的疾病修饰作用较小。重要的是,治疗后对鲁索替尼的反应可能会丧失,这表明MPN克隆获得了耐药性。与其他酪氨酸激酶抑制剂一样,MPN患者中尚未描述耐药性突变,这表明功能过程重新激活了JAK2信号通路。绕过JAK2抑制的代偿性信号通路和其他过程导致MPN细胞的内在耐药性,从而限制了JAK2抑制的总体疗效。JAK2抑制与聚乙二醇化干扰素-α(一种成熟的MPN治疗方法)、B细胞淋巴瘤2抑制等的联合应用正在进行临床开发,有可能提高治疗效果。临床上正在研究针对JAK2以外其他分子的新型单药治疗方法。应特别关注贫血和血小板减少的骨髓纤维化患者,这是一个急需治疗选择的脆弱患者群体。新治疗方法的范围不断扩大,将增加MPN患者的治疗选择。这就要求我们同时提高对MPN生物学的认识,为个体MPN患者制定量身定制的治疗策略提供依据。