Lingervelder Deon, Koffijberg Hendrik, Kusters Ron, IJzerman Maarten J
Health Technology and Services Research Department, Technical Medical Centre, University of Twente, P.O. Box 217, Enschede, 7500 AE, The Netherlands.
Laboratory for Clinical Chemistry and Haematology, Jeroen Bosch Hospital, 's Hertogenbosch, The Netherlands.
Pharmacoecon Open. 2021 Jun;5(2):157-173. doi: 10.1007/s41669-020-00248-1. Epub 2021 Jan 6.
Point-of-care testing (POCT) has become an essential diagnostic technology for optimal patient care. Its implementation, however, still falls behind. This paper reviews the available evidence on the health economic impact of introducing POCT to assess if poor POCT uptake may be related to lacking evidence.
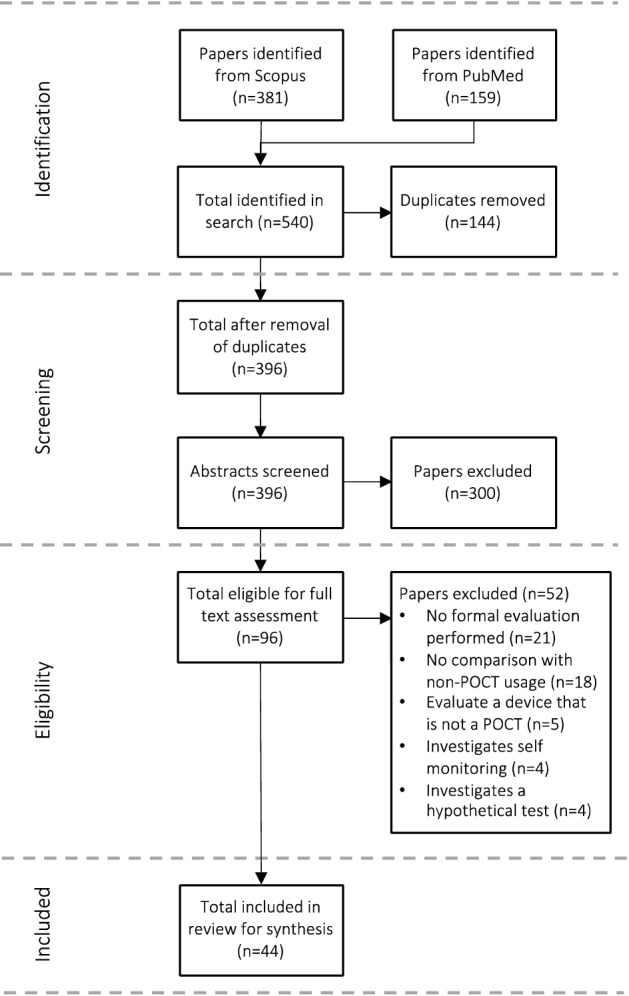
The Scopus and PubMed databases were searched to identify publications describing a health economic evaluation of a point-of-care (POC) test. Data were extracted from the included publications, including general and methodological characteristics as well as the study results summarized in either cost, effects or an incremental cost-effectiveness ratio. Results were sorted into six groups according to the POC test's purpose (diagnosis, screening or monitoring) and care setting (primary care or secondary care). The reporting quality of the publications was determined using the CHEERS checklist.
The initial search resulted in 396 publications, of which 44 met the inclusion criteria. Most of the evaluations were performed in a primary care setting (n = 31; 70.5%) compared with a secondary care setting (n = 13; 29.5%). About two thirds of the evaluations were on POC tests implemented with a diagnostic purpose (n = 28; 63.6%). More than 75% of evaluations concluded that POCT is recommended for implementation, although in some cases only under specific circumstances and conditions. Compliance with the CHEERS checklist items ranged from 20.8% to 100%, with an average reporting quality of 72.0%.
There were very few evaluations in this review that advised against the implementation of POCT. However, the uptake of POCT in many countries remains low. Even though the evaluations included in this review did not always include the full long-term benefits of POCT, it is clear that health economic evidence across a few dimensions of value already indicate the benefits of POCT. This suggests that the lack of evidence on POCT is not the primary barrier to its implementation and that the low uptake of these tests in clinical practice is due to (a combination of) other barriers. In this context, aspects around organization of care, support of clinicians and quality management may be crucial in the widespread implementation of POCT.
即时检验(POCT)已成为实现最佳患者护理的一项重要诊断技术。然而,其应用仍相对滞后。本文回顾了有关引入POCT对健康经济影响的现有证据,以评估POCT应用不佳是否可能与证据不足有关。
检索Scopus和PubMed数据库,以识别描述即时检验(POC)健康经济评估的出版物。从纳入的出版物中提取数据,包括一般特征和方法学特征,以及以成本、效果或增量成本效益比总结的研究结果。根据POC测试的目的(诊断、筛查或监测)和护理环境(初级护理或二级护理)将结果分为六组。使用CHEERS清单确定出版物的报告质量。
初步检索得到396篇出版物,其中44篇符合纳入标准。与二级护理环境(n = 13;29.5%)相比,大多数评估在初级护理环境中进行(n = 31;70.5%)。约三分之二的评估针对以诊断为目的实施的POC测试(n = 28;63.6%)。超过75%的评估得出结论,建议实施POCT,尽管在某些情况下仅在特定情况和条件下。符合CHEERS清单项目的比例从20.8%到100%不等,平均报告质量为72.0%。
本综述中很少有评估建议不实施POCT。然而,POCT在许多国家的应用率仍然很低。尽管本综述纳入的评估并不总是包括POCT的全部长期益处,但很明显,从几个价值维度来看,健康经济证据已经表明了POCT的益处。这表明,POCT缺乏证据并非其应用的主要障碍,这些测试在临床实践中应用率低是由于其他障碍(或多种障碍的组合)。在这种情况下,护理组织、临床医生支持和质量管理等方面可能对POCT的广泛应用至关重要。