Bergen Centre for Ethics and Priority Setting, Department of Global Public Health and Primary Care, University of Bergen, Bergen, Norway.
Department of Pediatrics and Child health, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia.
Int J Equity Health. 2021 Jan 6;20(1):9. doi: 10.1186/s12939-020-01328-8.
Increasing the coverage of community-based treatment of childhood pneumonia (CCM) is part of the strategy to improve child survival, increase life-expectancy at birth and promote equity in Ethiopia. However, full coverage of CCM has not been reached in any regions of the country. There are no sub-national cost-effectiveness analyses available to inform decision makers on the most equitable scale up strategy.
Our first objective is to estimate the sub-national cost-effectiveness and the interindividual inequality impacts of scaling up CCM coverages to 90% in each region. Our second objective is to explore the costs, health effects, and geographical inequality impacts associated with three scale-up scenarios promoting different policy-aims: maximizing health, reducing geographical inequalities, and achieving 90% universal coverage.
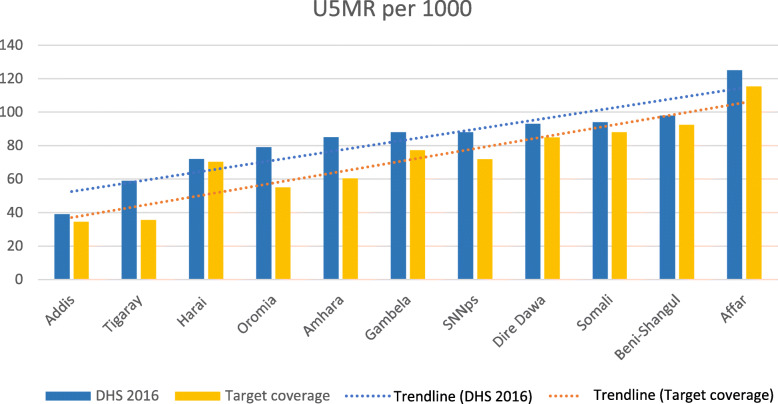
We used Markov modelling to estimate the sub-national cost-effectiveness of CCM in each region. All data were collected through literature review and adjusted to the region-specific proportions of the rural population. Health effects were modeled as life years gained and under-five deaths averted. Interindividual and geographical inequality impacts were measured by the GINI index applied to health. In scenario analysis we explored three different scale-up strategies: 1) maximizing health by prioritizing the regions where the intervention was the most cost-effective, 2) reducing geographical inequalities by prioritizing the regions with high baseline under-five mortality rate (U5MR), and 3) universal upscaling to 90% coverage in all the regions.
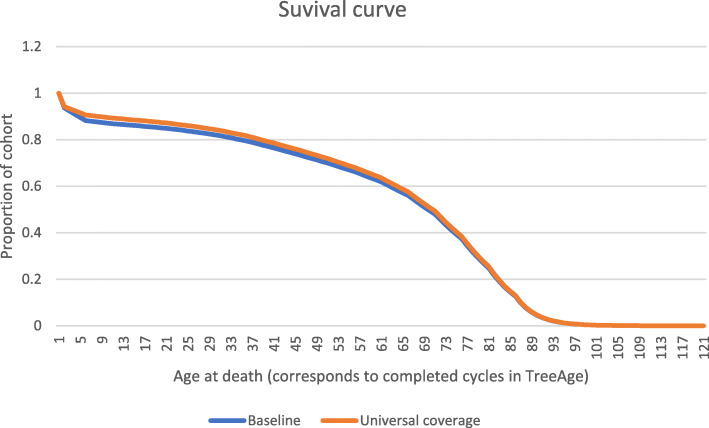
The regional incremental-cost effectiveness ratio (ICER) of scaling up the intervention coverage varied from 26 USD per life year gained in Addis to 199 USD per life year gained in the Southern Nations, Nationalities, and Peoples' region. Universal upscaling of CCM in all regions would cost about 1.3 billion USD and prevent about 90,000 under-five deaths. This is less than 15,000 USD per life saved and translates to an increase in life expectancy at birth of 1.6 years across Ethiopia. In scenario analysis, we found that prioritizing regions with high U5MR is effective in reducing geographical inequalities, although at the cost of fewer lives saved as compared to the health maximizing strategy.
Our model results illustrate a trade-off between maximizing health and reducing health inequalities, two common policy-aims in low-income settings.
提高社区儿童肺炎治疗(CCM)的覆盖率是提高儿童生存率、提高出生时预期寿命和促进埃塞俄比亚公平的战略的一部分。然而,该国任何地区都没有达到 CCM 的全面覆盖。没有关于在最公平的扩大规模战略方面为决策者提供信息的次国家级成本效益分析。
我们的第一个目标是估计扩大 CCM 覆盖范围至每个地区 90%的次国家级成本效益和个体间不平等影响。我们的第二个目标是探索与三种扩大规模方案相关的成本、健康效果和地理不平等影响,这些方案旨在实现不同的政策目标:最大化健康、减少地理不平等和实现 90%的普遍覆盖。
我们使用马尔可夫模型来估计每个地区 CCM 的次国家级成本效益。所有数据均通过文献综述收集,并根据农村人口的特定比例进行调整。健康效果被建模为获得的生命年数和避免的五岁以下儿童死亡人数。个体间和地理不平等影响通过应用于健康的基尼指数来衡量。在方案分析中,我们探索了三种不同的扩大规模策略:1)通过优先考虑干预措施最具成本效益的地区来最大化健康,2)通过优先考虑基线五岁以下儿童死亡率(U5MR)较高的地区来减少地理不平等,3)在所有地区普遍扩大规模至 90%的覆盖率。
扩大干预措施覆盖率的区域增量成本效益比(ICER)从在亚的斯亚贝巴每获得一个生命年的 26 美元到在南部民族、国家和人民地区每获得一个生命年的 199 美元不等。在所有地区普遍扩大 CCM 的规模将耗资约 13 亿美元,并防止约 90,000 名五岁以下儿童死亡。这不到每挽救一条生命的 15,000 美元,相当于埃塞俄比亚出生时预期寿命增加 1.6 年。在方案分析中,我们发现优先考虑 U5MR 较高的地区可以有效减少地理不平等,但与追求健康最大化的策略相比,挽救的生命更少。
我们的模型结果说明了在最大化健康和减少健康不平等之间的权衡,这是低收入国家的两个常见政策目标。