Health Systems Research Unit, South African Medical Research Council, Cape Town, South Africa.
School of Public Health, University of the Western Cape, Cape Town, South Africa.
J Glob Health. 2017 Jun;7(1):010403. doi: 10.7189/jogh.07.010403.
Sub-Saharan Africa still reports the highest rates of under-five mortality. Low cost, high impact interventions exist, however poor access remains a challenge. Integrated community case management (iCCM) was introduced to improve access to essential services for children 2-59 months through diagnosis, treatment and referral services by community health workers for malaria, pneumonia and diarrhea. This paper presents the results of an economic analysis of iCCM implementation in regions supported by UNICEF in six countries and assesses country-level scale-up implications. The paper focuses on costs to provider (health system and donors) to inform planning and budgeting, and does not cover cost-effectiveness.
The analysis combines annualised set-up costs and 1 year implementation costs to calculate incremental economic and financial costs per treatment from a provider perspective. Affordability is assessed by calculating the per capita financial cost of the program as a percentage of the public health expenditure per capita. Time and financial implications of a 30% increase in utilization were modeled. Country scale-up is modeled for all children under 5 in rural areas.
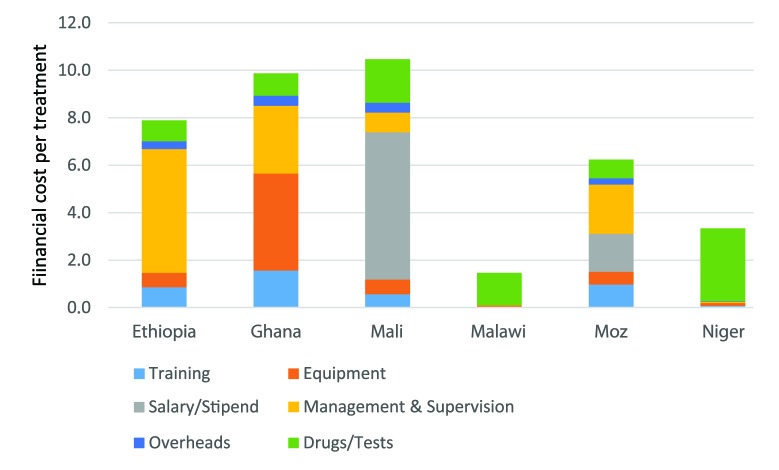
Utilization of iCCM services varied from 0.05 treatment/y/under-five in Ethiopia to over 1 in Niger. There were between 10 and 603 treatments/community health worker (CHW)/y. Consultation cost represented between 93% and 22% of economic costs per treatment influenced by the level of utilization. Weighted economic cost per treatment ranged from US$ 13 (2015 USD) in Ghana to US$ 2 in Malawi. CHWs spent from 1 to 9 hours a week on iCCM. A 30% increase in utilization would add up to 2 hours a week, but reduce cost per treatment (by 20% in countries with low utilization). Country scale up would amount to under US$ 0.8 per capita total population (US$ 0.06-US$0.74), between 0.5% and 2% of public health expenditure per capita but 8% in Niger.
iCCM addresses unmet needs and impacts on under 5 mortality. An economic cost of under US$ 1/capita/y represents a sound investment. Utilization remains low however, and strategies must be developed as a priority to improve demand. Continued donor support is required to sustain iCCM services and strengthen its integration within national health systems.
撒哈拉以南非洲地区报告的五岁以下儿童死亡率仍然最高。尽管存在低成本、高影响力的干预措施,但获得服务的机会仍然有限。综合社区病例管理(iCCM)的引入旨在通过社区卫生工作者为 2-59 个月大的儿童提供疟疾、肺炎和腹泻的诊断、治疗和转介服务,改善获得基本服务的机会。本文介绍了在六个国家由儿基会支持的区域实施 iCCM 的经济分析结果,并评估了国家层面的扩大规模影响。本文重点从提供者(卫生系统和捐助者)的角度介绍了计算每次治疗的增量经济和财务成本的年度化设立成本和 1 年实施成本,不包括成本效益。
分析结合了年度设立成本和 1 年实施成本,从提供者的角度计算每次治疗的增量经济和财务成本。通过计算方案的人均财政成本占人均公共卫生支出的百分比来评估可负担性。还对利用率增加 30%的时间和财务影响进行了建模。对农村地区所有 5 岁以下儿童进行了国家扩大规模的建模。
iCCM 服务的利用率从埃塞俄比亚的每名五岁以下儿童每年 0.05 次治疗到尼日尔的 1 次以上不等。每个社区卫生工作者(CHW)的治疗次数在 10 到 603 次之间。咨询费用占每次治疗经济成本的 93%至 22%,受利用率水平的影响。加权经济成本从加纳的每名治疗费用 13 美元(2015 年美元)到马拉维的 2 美元不等。CHW 每周花 1 到 9 小时用于 iCCM。利用率增加 30%将每周增加 2 小时,但会降低每次治疗的成本(在利用率低的国家降低 20%)。国家扩大规模的总成本将低于每人 0.8 美元(0.06-0.74 美元),占人均公共卫生支出的 0.5%至 2%,但在尼日尔占 8%。
iCCM 满足了未满足的需求,并对五岁以下儿童死亡率产生了影响。低于 1 美元/人/年的经济成本是合理的投资。然而,利用率仍然较低,因此必须优先制定战略来提高需求。需要继续得到捐助者的支持,以维持 iCCM 服务并加强其在国家卫生系统中的整合。