Korst Lisa M, Gregory Kimberly D, Nicholas Lisa A, Saeb Samia, Reynen David J, Troyan Jennifer L, Greene Naomi, Fridman Moshe
Childbirth Research Associates, LLC, North Hollywood, CA, USA.
Department of Obstetrics and Gynecology, Cedars-Sinai Medical Center, Burns Allen Research Institute, Los Angeles, CA, USA.
Matern Health Neonatol Perinatol. 2021 Jan 6;7(1):3. doi: 10.1186/s40748-020-00123-1.
Current interest in using severe maternal morbidity (SMM) as a quality indicator for maternal healthcare will require the development of a standardized method for estimating hospital or regional SMM rates that includes adjustment and/or stratification for risk factors.
To perform a scoping review to identify methodological considerations and potential covariates for risk adjustment for delivery-associated SMM.
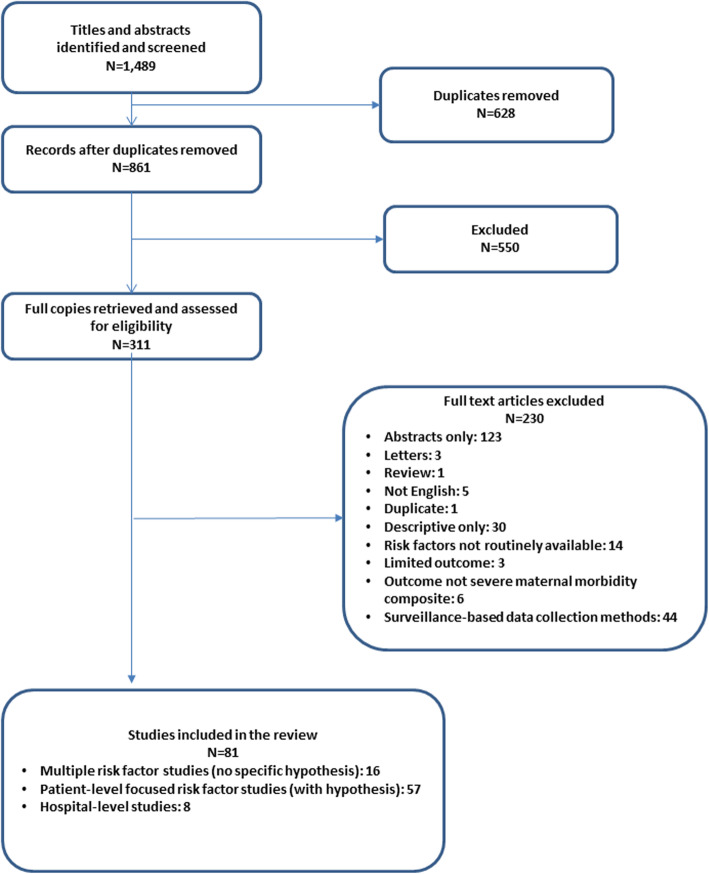
Following the guidelines for Preferred Reporting Items for Systematic Reviews and Meta-analyses Extension for Scoping Reviews, systematic searches were conducted with the entire PubMed and EMBASE electronic databases to identify publications using the key term "severe maternal morbidity."
Included studies required population-based cohort data and testing or adjustment of risk factors for SMM occurring during the delivery admission. Descriptive studies and those using surveillance-based data collection methods were excluded.
Information was extracted into a pre-defined database. Study design and eligibility, overall quality and results, SMM definitions, and patient-, hospital-, and community-level risk factors and their definitions were assessed.
Eligibility criteria were met by 81 studies. Methodological approaches were heterogeneous and study results could not be combined quantitatively because of wide variability in data sources, study designs, eligibility criteria, definitions of SMM, and risk-factor selection and definitions. Of the 180 potential risk factors identified, 41 were categorized as pre-existing conditions (e.g., chronic hypertension), 22 as obstetrical conditions (e.g., multiple gestation), 22 as intrapartum conditions (e.g., delivery route), 15 as non-clinical variables (e.g., insurance type), 58 as hospital-level variables (e.g., delivery volume), and 22 as community-level variables (e.g., neighborhood poverty).
The development of a risk adjustment strategy that will allow for SMM comparisons across hospitals or regions will require harmonization regarding: a) the standardization of the SMM definition; b) the data sources and population used; and c) the selection and definition of risk factors of interest.
当前将严重孕产妇发病率(SMM)用作孕产妇保健质量指标的关注,将需要开发一种标准化方法来估算医院或地区的SMM率,该方法包括对风险因素进行调整和/或分层。
进行一项范围综述,以确定与分娩相关的SMM风险调整的方法学考虑因素和潜在协变量。
按照系统评价和Meta分析扩展的范围综述的首选报告项目指南,使用整个PubMed和EMBASE电子数据库进行系统检索,以识别使用关键词“严重孕产妇发病率”的出版物。
纳入的研究需要基于人群的队列数据,以及对分娩入院期间发生的SMM风险因素进行测试或调整。排除描述性研究和使用基于监测的数据收集方法的研究。
信息被提取到一个预定义的数据库中。评估了研究设计和入选标准、总体质量和结果、SMM定义,以及患者、医院和社区层面的风险因素及其定义。
81项研究符合入选标准。方法学方法各不相同,由于数据源、研究设计、入选标准、SMM定义以及风险因素选择和定义存在广泛差异,研究结果无法进行定量合并。在确定的180个潜在风险因素中,41个被归类为既往疾病(如慢性高血压),22个为产科情况(如多胎妊娠),22个为产时情况(如分娩方式),15个为非临床变量(如保险类型),58个为医院层面变量(如分娩量),22个为社区层面变量(如社区贫困)。
要制定一种能够实现不同医院或地区间SMM比较的风险调整策略,需要在以下方面达成一致:a)SMM定义的标准化;b)所使用的数据源和人群;c)感兴趣的风险因素的选择和定义。