Klinik für Herz- und Kreislauferkrankungen Deutsches Herzzentrum MünchenTechnische Universität München Munich Germany.
1. Medizinische Klinik Klinikum rechts der IsarTechnische Universität München Munich Germany.
J Am Heart Assoc. 2021 Jan 19;10(2):e018304. doi: 10.1161/JAHA.120.018304. Epub 2021 Jan 7.
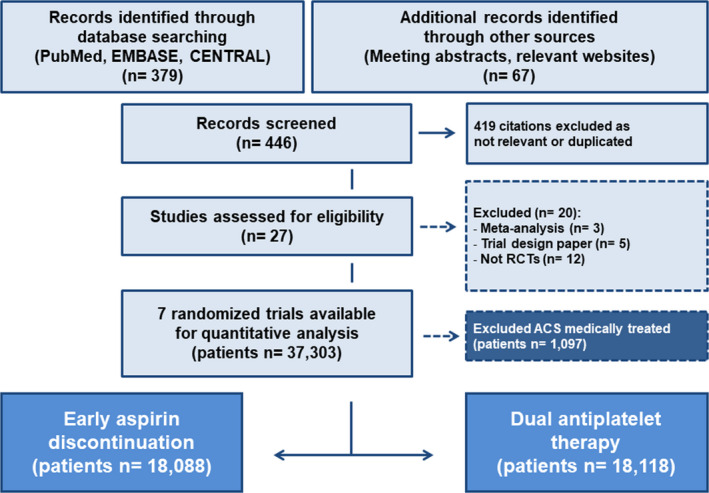
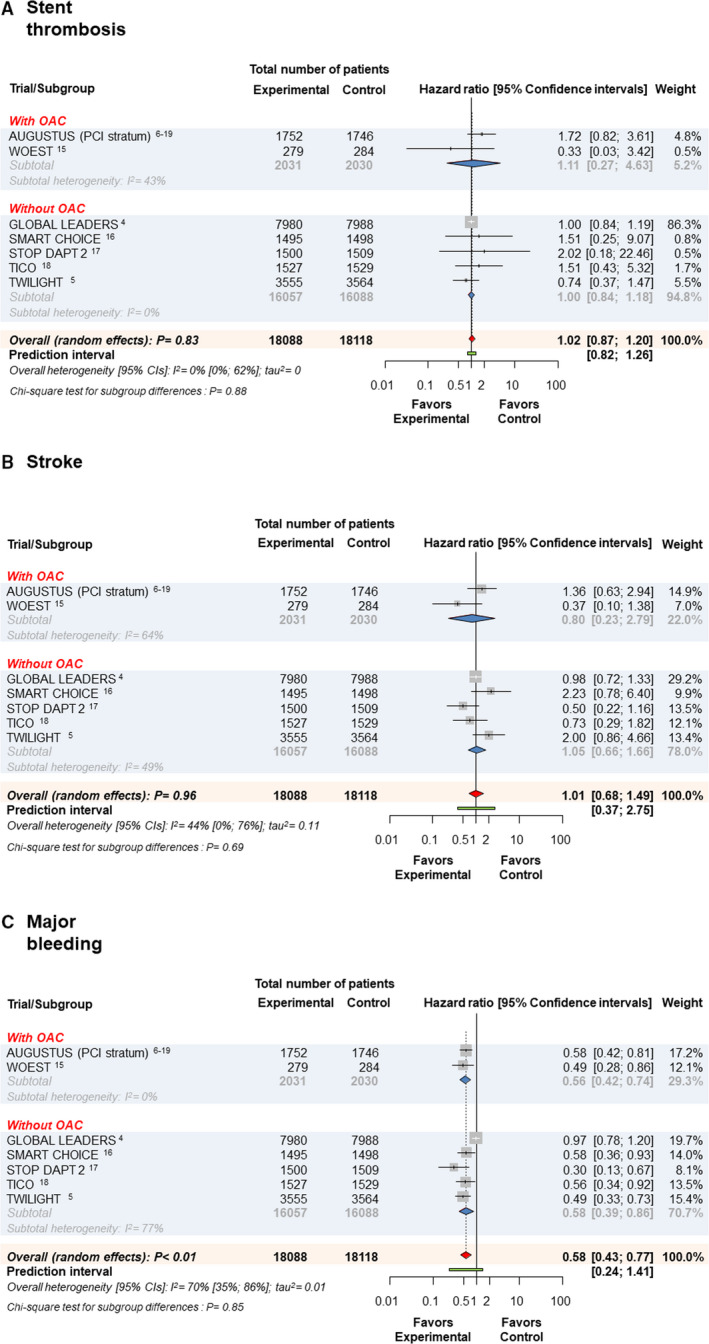
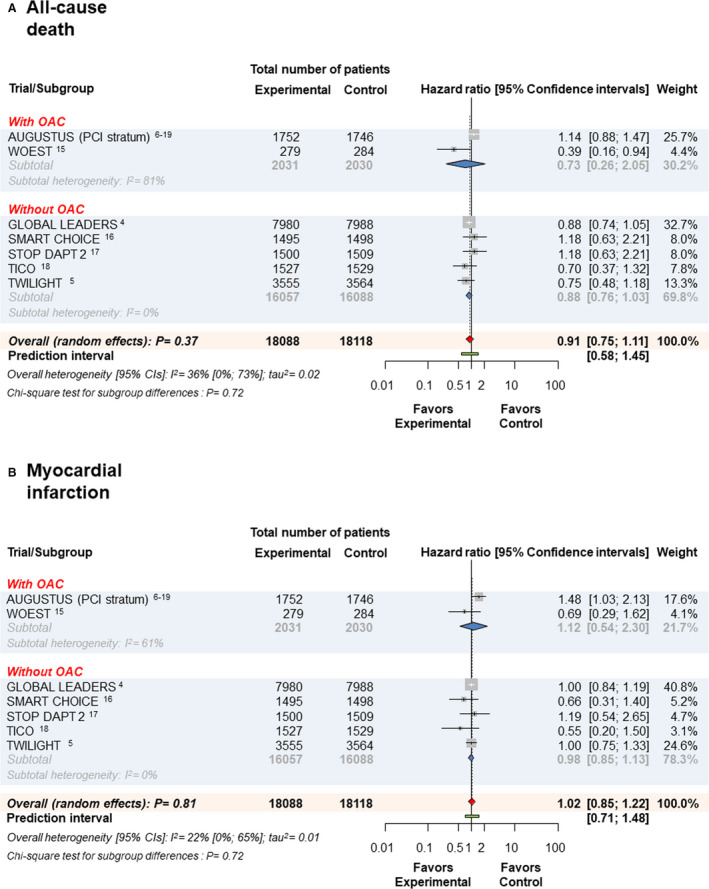
Background The clinical impact of early aspirin discontinuation compared with dual antiplatelet therapy (DAPT) in patients undergoing percutaneous coronary intervention with stenting remains poorly studied. We investigated the clinical outcomes of patients assigned to either early aspirin discontinuation or DAPT after percutaneous coronary intervention with stenting. Methods and Results We performed a meta-analysis of aggregate data from randomized clinical trials enrolling participants receiving a percutaneous coronary intervention with stenting and assigned to either early aspirin discontinuation or DAPT. Scientific databases were searched from inception through March 30, 2020. Trial-level hazard ratios (HRs) and 95% CIs were pooled using a random effects model with inverse variance weighting. The primary outcome was all-cause death. Secondary outcomes were myocardial infarction, stent thrombosis, stroke, and major bleeding. Overall, 36 206 participants were allocated to either early aspirin discontinuation (experimental therapy, n=18 088) or DAPT (control therapy, n=18 118) in 7 trials. Median follow-up was 12 months. All-cause death occurred in 2.5% of patients assigned to experimental and 2.9% of patients assigned control therapy (hazard ratio [HR], 0.91, 95% CI, 0.75-1.11; =0.37). Overall, patients treated with experimental versus control therapy showed no significant difference in terms of myocardial infarction (HR, 1.02 [0.85-1.22], =0.81), stent thrombosis (HR, 1.02 [0.87-1.20], =0.83), or stroke (HR, 1.01 [0.68-1.49], =0.96). However, the risk for major bleeding (HR, 0.58 [0.43-0.77], <0.01) was significantly reduced by experimental as compared with control therapy. Conclusions In patients treated with percutaneous coronary intervention and stenting, assigned to a strategy of early aspirin discontinuation versus DAPT, the risk of death and ischemic events is not significantly different but the risk of bleeding is lower.
与双联抗血小板治疗(DAPT)相比,经皮冠状动脉介入治疗(PCI)后早期阿司匹林停药对患者的临床影响仍研究甚少。我们研究了接受 PCI 并接受阿司匹林早期停药或 DAPT 的患者的临床结局。
我们对接受 PCI 并接受阿司匹林早期停药或 DAPT 的患者进行了汇总数据的荟萃分析。从研究开始到 2020 年 3 月 30 日,检索了科学数据库。使用随机效应模型和倒数方差加权法汇总试验水平的危险比(HR)和 95%CI。主要结局为全因死亡。次要结局为心肌梗死、支架血栓形成、卒中和大出血。共有 7 项试验纳入 36206 名患者,分别接受阿司匹林早期停药(试验治疗,n=18088)或 DAPT(对照治疗,n=18118)。中位随访时间为 12 个月。阿司匹林早期停药组和对照组的全因死亡发生率分别为 2.5%和 2.9%(HR,0.91,95%CI,0.75-1.11;=0.37)。总的来说,与对照组相比,接受试验治疗的患者在心肌梗死(HR,1.02[0.85-1.22],=0.81)、支架血栓形成(HR,1.02[0.87-1.20],=0.83)或卒中等方面没有显著差异(HR,1.01[0.68-1.49],=0.96)。然而,与对照组相比,试验组大出血的风险(HR,0.58[0.43-0.77],<0.01)显著降低。
在接受 PCI 和支架置入治疗的患者中,与 DAPT 相比,阿司匹林早期停药策略的死亡和缺血性事件风险无显著差异,但出血风险较低。