Abrard Stanislas, Fouquet Olivier, Riou Jérémie, Rineau Emmanuel, Abraham Pierre, Sargentini Cyril, Bigou Yannick, Baufreton Christophe, Lasocki Sigismond, Henni Samir
Department of Anesthesiology and Intensive Care, University Hospital of Angers, Angers, France.
Vascular Medicine, University Hospital of Angers, Angers, France.
Ann Intensive Care. 2021 Jan 7;11(1):4. doi: 10.1186/s13613-020-00789-y.
Cardiac surgery is known to induce acute endothelial dysfunction, which may be central to the pathophysiology of postoperative complications. Preoperative endothelial dysfunction could also be implicated in the pathophysiology of postoperative complications after cardiac surgery. However, the relationship between preoperative endothelial function and postoperative outcomes remains unknown. The primary objective was to describe the relationship between a preoperative microcirculatory dysfunction identified by iontophoresis of acetylcholine (ACh), and postoperative organ injury in patients scheduled for cardiac surgery using cardiopulmonary bypass (CPB).
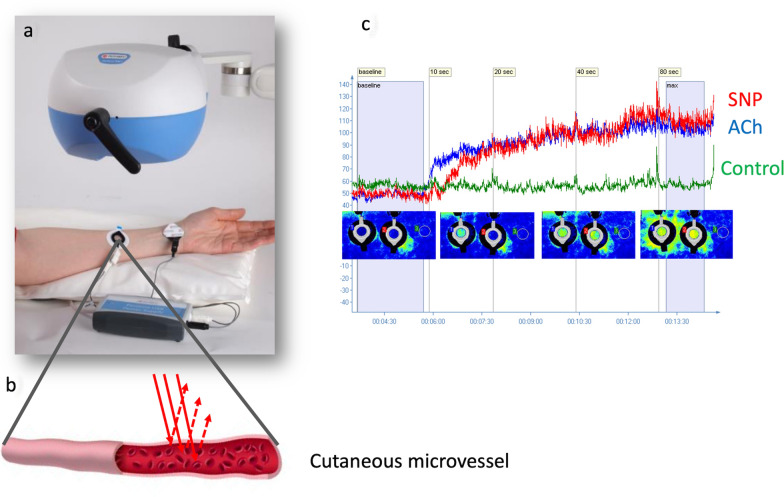
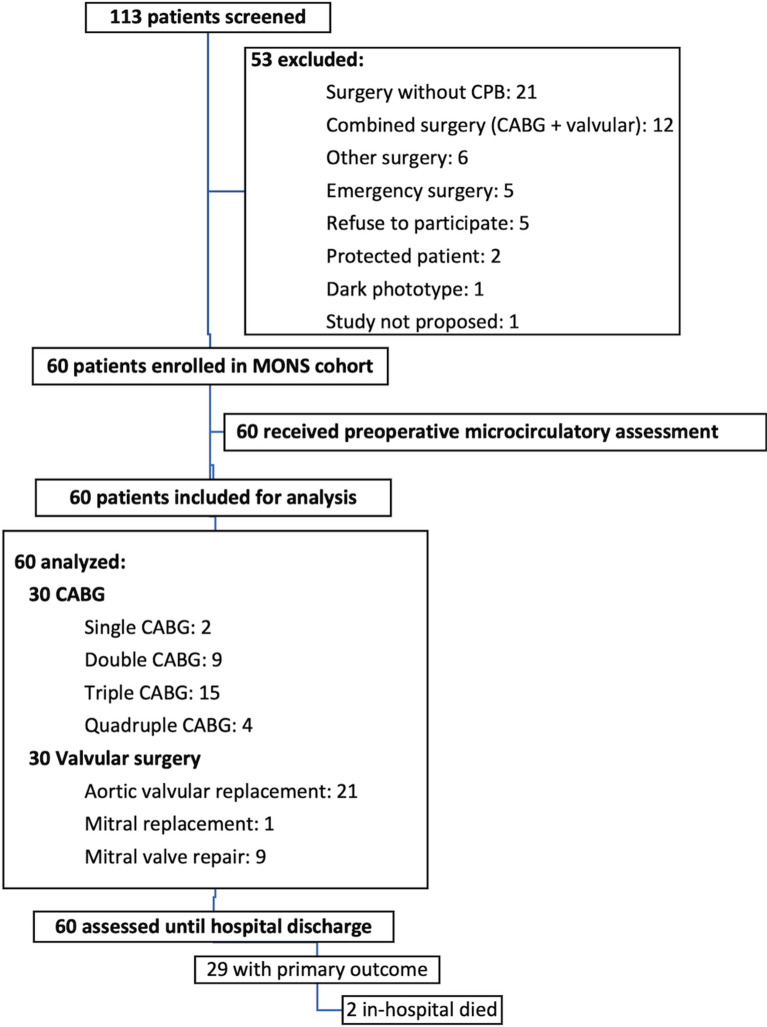
Sixty patients undergoing elective cardiac surgery using CPB were included in the analysis of a prospective, observational, single-center cohort study conducted from January to April 2019. Preoperative microcirculation was assessed with reactivity tests on the forearm (iontophoresis of ACh and nitroprusside). Skin blood flow was measured by laser speckle contrast imaging. Postoperative organ injury, the primary outcome, was defined as a Sequential Organ Failure Assessment score (SOFA) 48 h after surgery greater than 3.
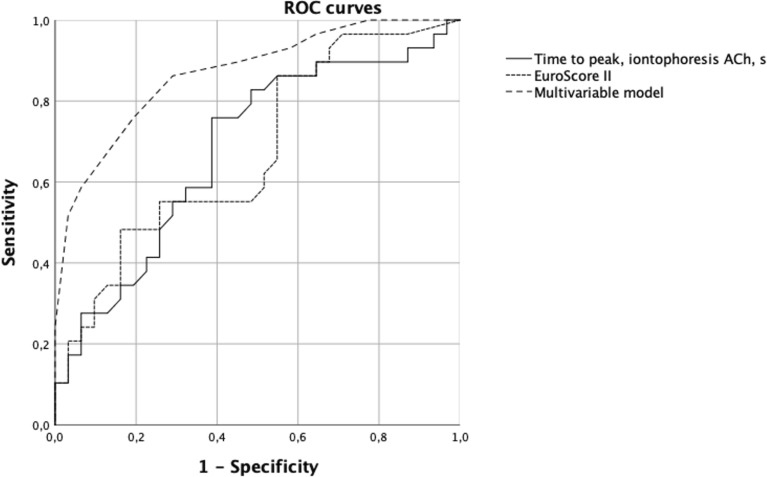
Organ injury at 48 h occurred in 29 cases (48.3%). Patients with postoperative organ injury (SOFA score > 3 at 48 h) had a longer time to reach the peak of preoperative iontophoresis of acetylcholine (133 s [104-156] vs 98 s [76-139] than patients without, P = 0.016), whereas endothelium-independent vasodilation to nitroprusside was similar in both groups. Beyond the proposed threshold of 105 s for time to reach the peak of preoperative endothelium-dependent vasodilation, three times more patients presented organ dysfunction at 48 h (76% vs 24% below or equal 105 s). In multivariable model, the time to reach the peak during iontophoresis of acetylcholine was an independent predictor of postoperative organ injury (odds ratio = 4.81, 95% confidence interval [1.16-19.94]; P = 0.030).
Patients who postoperatively developed organ injury (SOFA score > 3 at 48 h) had preoperatively a longer time to reach the peak of endothelium-dependent vasodilation. Trial registration Clinical-Trials.gov, NCT03631797. Registered 15 August 2018, https://clinicaltrials.gov/ct2/show/NCT03631797.
心脏手术已知会引发急性内皮功能障碍,这可能是术后并发症病理生理学的核心。术前内皮功能障碍也可能与心脏手术后的术后并发症病理生理学有关。然而,术前内皮功能与术后结局之间的关系仍不清楚。主要目的是描述通过乙酰胆碱(ACh)离子电渗疗法确定的术前微循环功能障碍与计划进行体外循环(CPB)心脏手术患者术后器官损伤之间的关系。
纳入2019年1月至4月进行的一项前瞻性、观察性、单中心队列研究分析的60例接受CPB择期心脏手术的患者。术前通过前臂反应性测试(ACh和硝普钠离子电渗疗法)评估微循环。通过激光散斑对比成像测量皮肤血流。术后器官损伤作为主要结局,定义为术后48小时序贯器官衰竭评估(SOFA)评分大于3。
48小时时发生器官损伤的有29例(48.3%)。术后发生器官损伤的患者(48小时时SOFA评分>3)达到术前乙酰胆碱离子电渗疗法峰值的时间比未发生器官损伤的患者更长(133秒[104 - 156]对98秒[76 - 139],P = 0.016),而两组对硝普钠的非内皮依赖性血管舒张相似。超过术前内皮依赖性血管舒张峰值时间的提议阈值105秒后,48小时时出现器官功能障碍的患者增加了两倍(76%对低于或等于105秒的24%)。在多变量模型中,乙酰胆碱离子电渗疗法达到峰值的时间是术后器官损伤的独立预测因素(比值比 = 4.81,95%置信区间[1.16 - 19.94];P = 0.030)。
术后发生器官损伤的患者(48小时时SOFA评分>3)术前达到内皮依赖性血管舒张峰值的时间更长。试验注册ClinicalTrials.gov,NCT03631797。2018年8月15日注册,https://clinicaltrials.gov/ct2/show/NCT03631797。