Veterans Health Administration-Tennessee Valley Healthcare System Geriatric Research, Education and Clinical Center (GRECC), Nashville, TN, USA.
Division of Hematology/Oncology, Department of Medicine, Vanderbilt University Medical Center, 2525 West End Ave., Suite 1200, Nashville, TN, 37203, USA.
BMC Health Serv Res. 2021 Jan 7;21(1):33. doi: 10.1186/s12913-020-06016-5.
A systems-level approach to smoking cessation treatment may optimize healthcare provider adherence to guidelines. Institutions such as the Veterans Health Administration (VHA) are unique in their systematic approach, but comparisons of provider behavior in different healthcare systems are limited.
We surveyed general medicine providers and specialists in a large academic health center (AHC) and its affiliated VHA in the Mid-South in 2017 to determine the cross-sectional association of healthcare system in which the provider practiced (exposure: AHC versus VHA) with self-reported provision of evidence-based smoking cessation treatment (delivery of counseling plus smoking cessation medication or referral) at least once in the past 12 months (composite outcome). Multivariable logistic regression with adjustment for specialty was performed in 2017-2019.
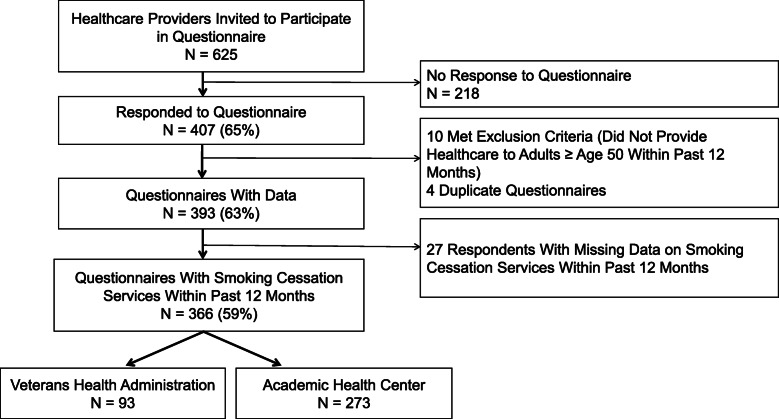
Of 625 healthcare providers surveyed, 407 (65%) responded, and 366 (59%) were analyzed. Most respondents practiced at the AHC (273[75%] vs VHA 93[25%]) and were general internists (215[59%]); pulmonologists (39[11%]); hematologists/oncologists (69[19%]); and gynecologists (43[12%]). Most respondents (328[90%]) reported the primary outcome. The adjusted odds of evidence-based smoking cessation treatment were higher among VHA vs. AHC healthcare providers (aOR = 4.3; 95% CI 1.3-14.4; p = .02). Health systems differed by provision of individual treatment components, including smoking cessation medication use (98% VHA vs. 90% AHC, p = 0.02) and referral to smoking cessation services (91% VHA vs. 65% AHC p = 0.001).
VHA healthcare providers were significantly more likely to provide evidence-based smoking cessation treatment compared to AHC healthcare providers. Healthcare systems' prioritization of and investment in smoking cessation treatment is critical to improving providers' adherence to guidelines.
采用系统方法进行戒烟治疗可能会提高医疗保健提供者对指南的依从性。退伍军人健康管理局(VHA)等机构在系统方法方面独具特色,但不同医疗体系中提供者行为的比较有限。
我们于 2017 年在中南部的一所大型学术医疗中心(AHC)及其附属 VHA 中调查了普通内科医生和专家,以确定提供者所在医疗体系(暴露:AHC 与 VHA)与自我报告的在过去 12 个月内至少提供一次基于证据的戒烟治疗(提供咨询加戒烟药物或转诊)的横断面关联(复合结局)。2017-2019 年进行了调整专业的多变量逻辑回归。
在接受调查的 625 名医疗保健提供者中,有 407 名(65%)做出了回应,其中 366 名(59%)进行了分析。大多数受访者在 AHC 执业(273[75%]对 VHA 93[25%]),并为普通内科医生(215[59%]);肺科医生(39[11%]);血液科/肿瘤科医生(69[19%]);和妇科医生(43[12%])。大多数受访者(328[90%])报告了主要结果。与 AHC 医疗保健提供者相比,VHA 医疗保健提供者提供基于证据的戒烟治疗的可能性更高(调整优势比[OR] = 4.3;95%置信区间[CI] 1.3-14.4;p = .02)。不同的医疗体系在个别治疗成分的提供方面存在差异,包括戒烟药物的使用(98% VHA 与 90% AHC,p = .02)和向戒烟服务的转诊(91% VHA 与 65% AHC,p = .001)。
与 AHC 医疗保健提供者相比,VHA 医疗保健提供者更有可能提供基于证据的戒烟治疗。医疗体系对戒烟治疗的重视和投资对于提高提供者对指南的依从性至关重要。